You have eczema and want to know whether peptides can calm the flares, itching, and barrier damage that creams alone do not fully control. Some peptides show promise for the two core problems in eczema: a weakened skin barrier and chronic inflammation. GHK-Cu (copper peptides) and KPV are the most discussed. But peptides are experimental for eczema, not a proven treatment, and they do not replace dermatologist-directed care.
| Quick Reference | Details |
|---|---|
| Do peptides cure eczema? | No; they may support barrier and inflammation |
| Barrier support | GHK-Cu (copper peptides) |
| Anti-inflammatory interest | KPV |
| Evidence level | Preliminary; not eczema-approved |
| Replace prescribed treatment? | No |
| Irritation risk | Real, especially on broken skin |
| FDA status | Not FDA-approved for eczema |
Peptides are not FDA-approved for eczema, and applying anything active to broken, inflamed skin carries irritation risk. This guide explains the rationale and the limits honestly. It is educational, not medical advice. Work with a dermatologist, especially for moderate or severe eczema.
For skin background, see what do peptides do for skin and GHK-Cu benefits.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Eczema Is Hard to Treat and Where Peptides Fit
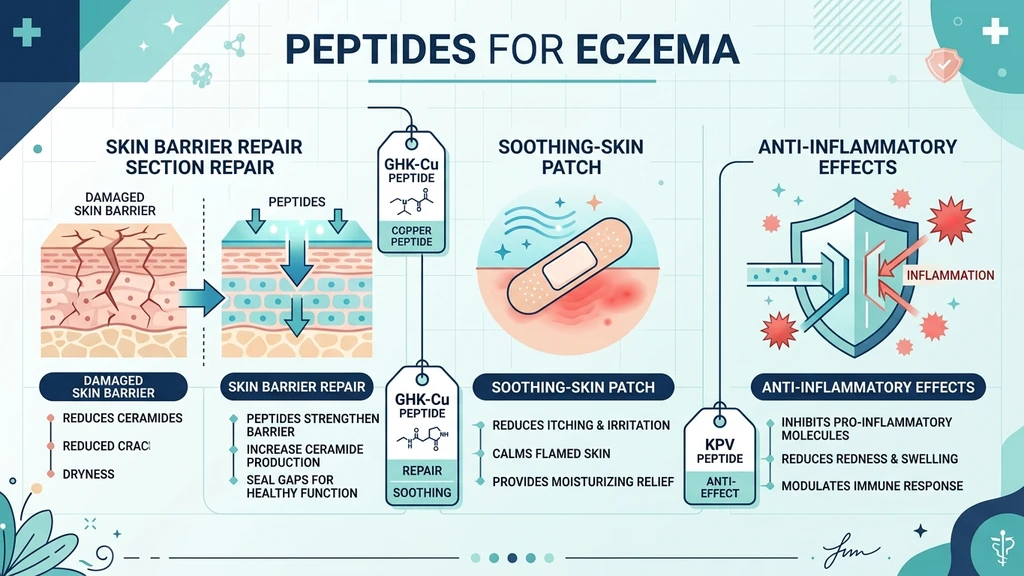
Eczema (atopic dermatitis) has two intertwined problems: a defective skin barrier that lets moisture out and irritants in, and an overactive inflammatory immune response that drives itching and flares. Effective treatment has to address both.
Think of the skin barrier as a brick wall again, with skin cells as bricks and lipids as mortar. In eczema, the mortar is faulty, so the wall leaks. Water escapes, allergens and microbes get in, and the immune system reacts, perpetuating a cycle of itch, scratch, and inflammation.
This is where peptides theoretically fit. Some peptides support skin remodeling and barrier function (the wall), and some have anti-inflammatory signaling activity (the immune overreaction). In principle, a peptide that helps rebuild the barrier and one that calms inflammation could address eczema's two root problems.
In practice, the evidence is early and indirect. Most peptide research relevant to eczema comes from wound healing and inflammation models, not eczema trials. The rationale is sound; the proof is thin. That gap is the central honest point of this guide. See our peptide safety guide.
GHK-Cu (Copper Peptides) for the Skin Barrier
GHK-Cu is the most evidence-backed peptide for skin generally, which is why it comes up for eczema. Its documented activities map onto what eczema-damaged skin needs.
GHK-Cu stimulates collagen and glycosaminoglycan synthesis, supports skin remodeling, and has antioxidant and tissue-repair properties (Pickart & Margolina, Int J Mol Sci, 2018). These barrier-supporting actions are the rationale for trying it on compromised skin.
The important caveat: most GHK-Cu research is on aging, wound healing, and cosmetic skin remodeling, not eczema specifically. Applying it to actively inflamed, broken eczema skin is different from applying it to intact skin, and it can sting or irritate.
If you try GHK-Cu for eczema-prone skin, the cautious approach is to use it on calm, intact skin between flares rather than on raw, weeping lesions, start at a low concentration, and patch test first. Copper peptides can backfire on sensitive skin, which is well-documented. See copper peptides ruined my skin and GHK-Cu side effects before using it anywhere near eczema.
KPV for Inflammation
KPV is a short peptide (a fragment of alpha-melanocyte-stimulating hormone) studied for anti-inflammatory activity. Because eczema is fundamentally inflammatory, KPV draws interest for calming the immune overreaction side of the disease.
Research on KPV has focused on its anti-inflammatory effects in models of gut and skin inflammation, where it appears to downregulate inflammatory signaling. This is the basis for the theory that it could help inflammatory skin conditions like eczema.
The reality check is the same as for GHK-Cu: the human evidence specifically for eczema is limited. KPV is used in research and by some for gut and inflammatory conditions, but it is not an established eczema treatment, and topical versus systemic delivery raises additional unknowns. See our KPV peptide dosage and KPV peptide morning or night guides.
Treat KPV for eczema as experimental. The anti-inflammatory rationale is plausible, but you would be extrapolating from non-eczema research. If you explore it, do so with medical guidance and modest expectations. For how peptides influence inflammation broadly, see peptides for inflammation.
What the Evidence Actually Shows
It is worth being blunt about the state of the science, because eczema is a condition where chasing unproven remedies can waste time and worsen skin.
What is established: GHK-Cu supports skin remodeling and barrier components in non-eczema contexts. KPV shows anti-inflammatory activity in research models. Both rationales connect logically to eczema's two core problems.
What is not established: There are no large, robust human trials proving that GHK-Cu or KPV treats eczema. The evidence is extrapolated from adjacent research, not direct.
What this means for you: Peptides may complement a proven eczema regimen for some people, but they are not a substitute for it, and they are not guaranteed to help. The first-line treatments, moisturizers and barrier repair, topical anti-inflammatories, trigger avoidance, and for moderate-to-severe cases prescription therapies, have strong evidence that peptides do not.
The responsible position: peptides for eczema are a reasonable experiment for some, layered on top of standard care, not a replacement. Anyone with moderate or severe eczema should be under dermatologist care, where newer prescription treatments may help far more than any research peptide. See what do peptides do for skin.
How to Use Peptides Safely on Eczema-Prone Skin
If you decide to try peptides as an adjunct, applying anything active to eczema skin demands extra caution. Broken skin absorbs and reacts differently than healthy skin.
Patch test first. Apply to a small area of intact skin for several days before broader use. Eczema skin is reactive, and a patch test catches problems early.
Use between flares, not on raw lesions. Active, weeping, or cracked eczema is the wrong canvas for an active peptide. Use peptides on calm, intact skin during maintenance phases.
Start low and infrequent. Low concentration, a few times a week, building only if tolerated.
Keep the foundation in place. Continue your moisturizer, barrier creams, and any prescribed treatments. Peptides are an addition, not a replacement.
Stop if it stings or worsens. Irritation on eczema skin escalates quickly. Discontinue at the first sign of worsening.
Check interactions. Do not layer peptides with strong actives that already irritate eczema skin. Use the peptide interaction checker.
Quantified guidance: a patch test over several days plus a low starting concentration prevents most avoidable reactions. If skin reacts even at low exposure, peptides are not right for your eczema. See GHK-Cu microneedling for why broken-skin delivery raises risk.
What Peptides Cannot Replace
The single most important section: peptides do not replace established eczema care. Substituting them for proven treatment can let eczema worsen.
Moisturizers and barrier repair. Daily emollients are the backbone of eczema management. Ceramide-rich moisturizers rebuild the faulty barrier. Nothing replaces them.
Prescribed anti-inflammatories. Topical corticosteroids and non-steroidal prescription options control flares with strong evidence. Peptides do not match this.
Trigger management. Identifying and avoiding personal triggers (irritants, allergens, stress, heat) does more than any topical for many people.
Dermatologist care for moderate-to-severe eczema. Newer systemic and biologic treatments have transformed severe eczema outcomes. These are in a different league from research peptides.
The honest hierarchy: foundation care and medical treatment first, peptides as an optional adjunct only after the basics are solid. Anyone tempted to drop their prescribed regimen in favor of peptides is making a mistake. Review our peptide safety guide and keep your dermatologist in the loop.
Common Mistakes With Peptides for Eczema
Mistake 1: Treating peptides as a cure. They may support barrier and inflammation but do not cure eczema. The fix: use them as an adjunct to proven care.
Mistake 2: Applying to raw, broken lesions. Active peptides on weeping eczema sting and can worsen it. The fix: use only on calm, intact skin between flares.
Mistake 3: Skipping the patch test. Eczema skin is reactive, and untested products cause avoidable flares. The fix: patch test for several days first.
Mistake 4: Dropping prescribed treatment. Replacing evidence-based care with peptides lets eczema worsen. The fix: keep moisturizers and prescribed treatments; add peptides only on top.
Mistake 5: Layering peptides with irritating actives. Stacking makes reactions worse and harder to diagnose. The fix: simplify and check the peptide interaction checker. See copper peptides ruined my skin for how this goes wrong.
Frequently Asked Questions
Can peptides help eczema?
Some peptides may support the two core problems in eczema: GHK-Cu for skin barrier repair and KPV for inflammation. But the evidence is preliminary and extrapolated from non-eczema research, so they are experimental, not proven treatments. They complement standard care rather than replacing it. See what do peptides do for skin.
Is GHK-Cu good for eczema?
GHK-Cu supports skin remodeling and barrier components, which is the rationale for trying it on eczema-prone skin. However, most research is on aging and wound healing, not eczema, and copper peptides can irritate sensitive or broken skin. Use only on calm, intact skin, start low, and patch test. See GHK-Cu benefits and copper peptides ruined my skin.
Does KPV reduce eczema inflammation?
KPV shows anti-inflammatory activity in research models, which is why it draws interest for inflammatory skin conditions like eczema. But human evidence specifically for eczema is limited, so it remains experimental. The anti-inflammatory rationale is plausible but not proven for this use. See our KPV peptide dosage guide.
Are peptides safe to use on eczema skin?
Applying active peptides to broken, inflamed eczema carries real irritation risk, since damaged skin absorbs and reacts differently. The safer approach is to use them only on calm, intact skin between flares, patch test first, start low, and stop at any sign of worsening. Keep your prescribed regimen in place. Review our peptide safety guide.
Can peptides replace my eczema cream or steroid?
No. Daily moisturizers, barrier repair, and prescribed anti-inflammatories have strong evidence that peptides do not match. Replacing proven treatment with experimental peptides can let eczema worsen. Use peptides only as an optional adjunct on top of established care, and keep your dermatologist informed.
How should I start peptides for eczema-prone skin?
Patch test on intact skin for several days, use a low concentration only on calm skin between flares, and apply a few times a week before building up. Keep your moisturizers and prescribed treatments going, avoid layering with irritating actives, and stop at the first sign of stinging or worsening. Check combinations with the peptide interaction checker.
Should I see a dermatologist before trying peptides?
Yes, especially for moderate or severe eczema. Newer prescription and biologic treatments have transformed eczema outcomes and far outperform research peptides. A dermatologist can build an evidence-based regimen and advise whether adding peptides as an adjunct makes sense for your skin. See peptides for inflammation for context.
The Bottom Line
Peptides for eczema target the right problems on paper. GHK-Cu supports the weakened skin barrier, and KPV has anti-inflammatory activity, addressing eczema's two root issues. The logic is sound, which is why interest is growing fast.
The science, though, is early. There are no robust human trials proving peptides treat eczema; the rationale is extrapolated from wound-healing and inflammation research. That makes them a reasonable experiment for some people as an adjunct, not a proven treatment and never a replacement for established care.
If you try peptides, treat eczema skin with extra caution: patch test, use only on calm intact skin between flares, start low, and keep your moisturizers and prescribed treatments going. For moderate or severe eczema, a dermatologist's regimen will help far more than any research peptide. Check combinations with the peptide interaction checker, review GHK-Cu benefits and its cautions, and always work with a healthcare provider.
Helpful Tools
Related Articles
Peptides for Psoriasis: The Evidence
Peptides for psoriasis: the honest evidence on KPV, GHK-Cu, BPC-157, and why LL-37 drives the disease rather than treating it. See a dermatologist.
KPV Peptide Benefits: What the Evidence Shows
KPV peptide benefits ranked by evidence: strong preclinical colitis data, plausible skin effects, weak systemic claims. No registered human trial exists.
KLOW Peptide: Benefits, Dosage, and KLOW vs GLOW
KLOW peptide benefits, blend composition (GHK-Cu, BPC-157, TB-500, KPV), per-component dosing math, the copper ceiling, and how KLOW differs from GLOW.
Copper Peptides Ruined My Skin: Why
Copper peptides ruined my skin? Why GHK-Cu can cause breakouts, redness, purging, and irritation, who is at risk, how to recover, and when to stop.