You paid $300 for the vial, and a forum thread says a quarter of the dose works nearly as well for a quarter of the price. Microdosing a GLP-1 means deliberately holding your dose below the range clinical trials tested. No trial has established that sub-therapeutic GLP-1 dosing produces meaningful weight loss. It is an off-label practice with no efficacy or safety data behind it.
| Quick Reference | Answer |
|---|---|
| What is microdosing GLP-1? | Dosing below the trial-tested therapeutic range on purpose |
| Is it clinically validated? | No. Zero trials of sub-therapeutic dosing for weight loss |
| Is it the same as titration? | No. Titration climbs toward a therapeutic dose |
| Main drivers | Drug cost and fear of nausea |
| Main risk | Paying full price and carrying side effects for little weight loss |
| Second risk | Dose math errors when splitting multi-dose vials |
| FDA position | No approved sub-therapeutic schedule for any GLP-1 |
| Safer alternative | A slower approved titration, supervised by a prescriber |
What follows describes the class across semaglutide, tirzepatide, retatrutide and liraglutide, and what the dose-response evidence actually shows. It is educational, not medical advice. Any dose change belongs to you and your prescriber.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Microdosing a GLP-1 Means
Every GLP-1 receptor agonist on the market was tested at a specific weekly dose, and that dose is what the weight loss numbers describe. Semaglutide 2.4 mg. Tirzepatide 5, 10 and 15 mg. Retatrutide 4, 8 and 12 mg in phase 2. Microdosing means choosing a dose beneath that range and staying there.
The doses people describe as microdoses cluster far below the tested range: 0.1 to 0.25 mg of semaglutide weekly, 0.5 to 2.5 mg of tirzepatide, sometimes stretched to a shot every ten or fourteen days. These numbers come from forums, telehealth marketing and compounding pharmacy price tiers. They come from no trial protocol.
The class-level point matters more than any single drug. Semaglutide is a GLP-1 agonist, tirzepatide adds GIP, and retatrutide adds glucagon on top of both. Their potency curves are different, so a "microdose" of one is not comparable to a "microdose" of another. Drug-specific numbers live in the tirzepatide microdosing chart and the guide to how to microdose semaglutide.
One thing to be clear about from the start. The absence of trial data does not mean microdosing is proven useless. It means nobody has looked. Anyone who tells you sub-therapeutic GLP-1 dosing "works fine" is describing an anecdote.
The Difference Between Titration and Microdosing
Every approved GLP-1 label opens with a low dose. Wegovy starts at 0.25 mg weekly. Zepbound starts at 2.5 mg. Saxenda starts at 0.6 mg daily. People read those starting doses and conclude the manufacturer built a microdose into the label.
That reading is backwards. The starting dose exists because the gut needs time to adapt. Rapid escalation to 2.4 mg of semaglutide produces nausea and vomiting severe enough to stop treatment, so the label climbs in four-week steps until the therapeutic dose is reached. The starting dose is a waypoint with an expiry date.
Zepbound's label says the plain part out loud: 2.5 mg once weekly is a treatment initiation dose and is not intended for glycemic control or maintenance. The schedule exists to deliver you to 5, 10 or 15 mg with a working stomach. See the semaglutide titration schedule for the full climb.
Microdosing inverts the purpose. It treats the on-ramp as the destination and parks there indefinitely. The dose is the same number; the intent, the duration and the expected outcome are entirely different.
Two people injecting 0.25 mg of semaglutide this week can be doing completely different things. One is four weeks from 0.5 mg. The other plans to inject 0.25 mg every week for a year.
Why a Quarter of the Dose Does Not Give a Quarter of the Result
Think about the knob on a shower. The first quarter turn away from cold barely changes anything: the water warms a little, and you are still not showering in it. The middle of the travel is where temperature moves fast, a few degrees per centimetre of rotation. Push past that and the last quarter turn adds almost nothing, because the water heater has hit its ceiling.
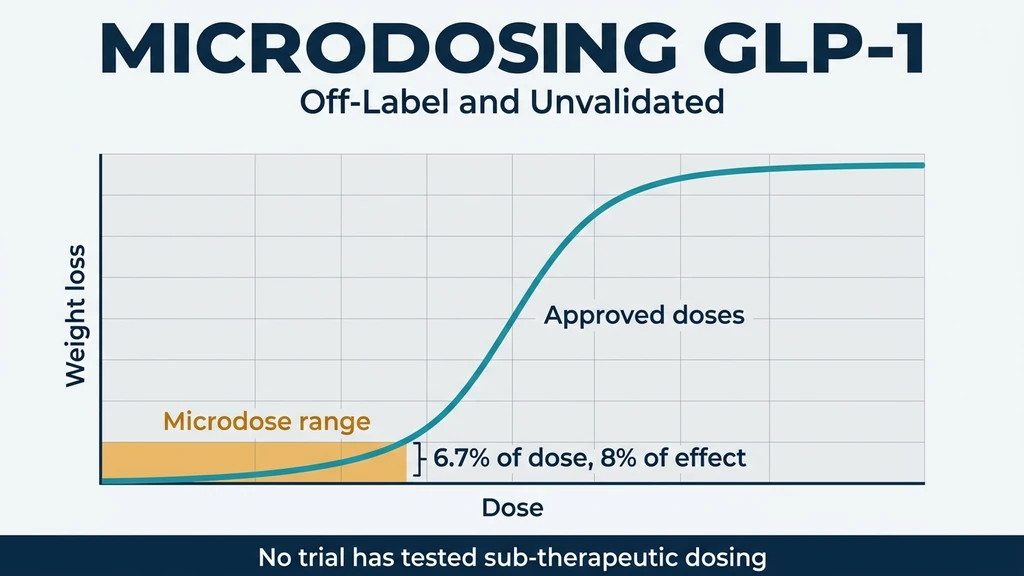
Drug effect follows the same shape. Plot response against dose and you get a sigmoid curve: a shallow foot, a steep middle, and a plateau. Sit on the foot and you spend the full effort for a fraction of the effect, because dose and response are not proportional anywhere on that curve.
The tirzepatide phase 2 data draws the foot precisely. Over 26 weeks, 1 mg weekly produced 0.9 kg of weight loss while 15 mg produced 11.3 kg (Frias et al., Lancet, 2018). The 1 mg dose is 6.7% of the maximum dose and delivers 8% of the weight loss. There is no bargain hidden on the foot of the curve.
Retatrutide behaves the same way. At 48 weeks the 1 mg group lost 8.7% of body weight and the 12 mg group lost 24.2% (Jastreboff et al., N Engl J Med, 2023). Triple agonism makes the foot of the curve less punishing, which is exactly why microdosing numbers borrowed from one drug tell you nothing about another.
Sub-therapeutic dosing does produce some effect. It produces less effect than the fraction of the dose would suggest, and no trial has measured whether that effect persists past the first few months.
Two Ways Microdosing Costs You: The Numbers
Scenario 1: you buy a full year of the foot of the curve.
You microdose tirzepatide at 1 mg weekly for 12 months to control appetite on a budget. Compounded tirzepatide runs roughly $250 to $400 a month, so the year costs $3,000 to $4,800. Based on the phase 2 dose-response, 1 mg weekly is the dose that produced 0.9 kg over 26 weeks, against 11.3 kg at 15 mg (Frias et al., Lancet, 2018).
You still get the side effects. GI symptoms appear at the starting doses, which is the entire reason the titration schedule exists. So the ledger reads: $4,800 spent, nausea tolerated, roughly 2 kg lost. Someone titrating to 10 mg over the same year would have paid a similar compounded price and landed in the range where trials recorded 19.5% body weight reduction (Jastreboff et al., N Engl J Med, 2022). The fix: price the outcome, not the milligram, before committing to a year of it.
Scenario 2: the reconstitution math doubles your dose.
Microdosing forces you into multi-dose vials and hand-drawn syringes, because no pen delivers 0.125 mg. You have a 5 mg semaglutide vial and intend to add 1 mL of bacteriostatic water, giving 5 mg/mL. Your 0.25 mg microdose is 0.05 mL, which is 5 units on a U-100 syringe.
You draw the diluent to the 50-unit mark instead of 100, adding 0.5 mL. Concentration is now 10 mg/mL. The same 5 units on the same syringe deliver 0.5 mg. You have doubled your dose and nothing about the injection looked different.
The FDA has logged this failure at far worse multiples. Reviewing adverse event reports for compounded semaglutide, the agency found the majority described patients drawing more than the prescribed dose from a multi-dose vial, administering five to 20 times the intended dose, with outcomes including vomiting, dehydration, fainting and acute pancreatitis. Confusion between millilitres, milligrams and units drove most of them.
The fix: reconstitute once, write the concentration on the vial in marker, and verify every conversion in the peptide unit converter before you draw.
The third cost is quieter. A compounded multi-dose vial carries a beyond-use date measured in weeks. Stretching a 5 mg vial across 20 microdoses means holding it far longer than a standard schedule would, puncturing the stopper repeatedly, and injecting from it after that date has passed.
How to Read a Dose-Response Curve
Every dose decision you will ever make is a point on a curve, and almost nobody teaches you to read one. The skill takes ten minutes to learn and it will change how you interpret every dosing claim you see online.
Dose runs along the bottom axis, usually on a logarithmic scale, so each step to the right multiplies rather than adds. Response runs up the side. The line joining them is an S: shallow at the left, steep through the middle, flat at the right. Pharmacologists call the dose that produces half the maximum response the ED50, and it sits at the steepest part of the climb.
Three regions, three practical meanings:
- 1.The foot. Real biology is happening. Receptors are binding. The measured outcome barely moves because too few receptors are occupied at any moment to change appetite, gastric emptying and insulin signalling enough to register on a scale.
- 2.The steep middle. Small dose increases buy large response increases. Every approved GLP-1 maintenance dose sits here or just past it. This is where a titration schedule is trying to deliver you.
- 3.The plateau. Receptors are saturated. Extra drug adds side effects and adds nothing else. This is why tirzepatide stops at 15 mg.
Now read a real trial as a curve. Daily semaglutide at 52 weeks produced 6.0% weight loss at 0.05 mg, 8.6% at 0.1 mg, 11.6% at 0.2 mg, 11.2% at 0.3 mg and 13.8% at 0.4 mg, against 2.3% on placebo (O'Neil et al., Lancet, 2018). Doubling from 0.05 to 0.1 mg bought 2.6 percentage points. Doubling again to 0.2 mg bought 3.0 more. Then the curve flattens: 0.3 mg scored slightly below 0.2 mg, and quadrupling the dose from 0.1 mg to 0.4 mg added only 5.2 points.
Read that curve carefully and the microdosing case gets weaker, not stronger. The cheapest dose on the list still needed a full 52 weeks to produce 6.0%, in a supervised trial, with lifestyle counselling attached. Nobody has run the equivalent study on 0.1 mg weekly, which is roughly a seventh of that daily exposure.
The habit to build: whenever someone quotes you a microdose, ask which trial arm that dose corresponds to and what that arm actually lost. If no arm exists, the number is invented. The semaglutide dosage calculator works from label doses for exactly this reason.
Approved Titration Schedules Across the GLP-1 Class
The left side of this table is regulator-approved and trial-backed. The right column is a description of reported off-label behaviour, collected from clinics and forums. It carries no efficacy or safety data and belongs in a different category from everything to its left.
| Drug | Class | Approved starting dose | Approved escalation | Trial-tested maintenance | Reported microdose range (unvalidated) |
|---|---|---|---|---|---|
| Semaglutide (Wegovy) | GLP-1 | 0.25 mg weekly | +1 step every 4 weeks: 0.5, 1.0, 1.7 | 2.4 mg weekly | 0.1 to 0.25 mg weekly, held indefinitely |
| Semaglutide (Ozempic) | GLP-1 | 0.25 mg weekly | 0.5 mg after 4 weeks, then 1.0, 2.0 | 0.5 to 2.0 mg weekly | 0.1 to 0.25 mg weekly, held indefinitely |
| Tirzepatide (Zepbound) | GIP + GLP-1 | 2.5 mg weekly, 4 weeks | +2.5 mg every 4 weeks minimum | 5, 10 or 15 mg weekly | 0.5 to 2.5 mg weekly, or 2.5 mg every 10 to 14 days |
| Liraglutide (Saxenda) | GLP-1 | 0.6 mg daily, week 1 | +0.6 mg weekly: 1.2, 1.8, 2.4 | 3.0 mg daily | 0.6 mg daily, held indefinitely |
| Retatrutide | GIP + GLP-1 + glucagon | Not approved | Phase 2 escalated from 2 or 4 mg in 4-week steps | 4, 8, 12 mg weekly (phase 2) | 1 to 2 mg weekly |
Weight loss at the tested maintenance doses: semaglutide 2.4 mg produced 14.9% at 68 weeks (Wilding et al., N Engl J Med, 2021), tirzepatide 15 mg produced 20.9% at 72 weeks (Jastreboff et al., N Engl J Med, 2022), and retatrutide 12 mg produced 24.2% at 48 weeks in phase 2 (Jastreboff et al., N Engl J Med, 2023). No comparable figure exists for any dose in the right-hand column.
Two more facts belong beside that table. Stopping a GLP-1 reverses the effect: participants who switched from semaglutide to placebo regained 6.9% of body weight over 48 weeks while those who continued lost a further 7.9% (Rubino et al., JAMA, 2021). Tirzepatide behaves identically, with 14% regain after withdrawal (Aronne et al., JAMA, 2024).
Those two trials are the closest evidence we have to a maintenance microdose question, and neither one tested a reduced dose. Both compared the full dose against nothing. Whether a low dose holds weight after a full-dose loss is an open question, and it is the single most interesting untested claim in this whole area. For what is known about staying on, see the tirzepatide maintenance dose after weight loss.
Liraglutide's 3.0 mg daily dose produced 8.4 kg of loss over 56 weeks (Pi-Sunyer et al., N Engl J Med, 2015), which is the weakest performance in the class and a reminder that potency differences between these drugs are large. Dividing a weak drug further leaves very little.
The Two Real Reasons People Microdose, and What Actually Solves Them
Nobody microdoses because they read a paper. They microdose because of money or because of nausea, and both problems have answers that do not require abandoning the tested dose.
Cost. A branded GLP-1 without insurance runs into four figures a year, and the arithmetic of splitting a vial is seductive. The honest accounting includes the outcome: money spent on a dose that produces 0.9 kg is money spent for nothing, while money spent reaching a therapeutic dose buys a documented result. Compare real prices in the GLP-1 cost statistics before you decide that a smaller dose is the cheaper path.
Nausea. GI symptoms hit hardest during escalation and fade with time on dose. The approved answer is a slower climb rather than a permanent stop. Prescribers routinely hold a patient at 0.25 mg or 2.5 mg for eight or twelve weeks instead of four, which is off-label in duration but keeps the destination intact. Symptom management is documented in how to relieve nausea from semaglutide.
The difference between a slow titration and a microdose is a prescriber, a plan and a date. One of them ends at a dose that trials have validated. The other has no end.
There is also the question of what is actually in the vial. Sub-therapeutic dosing almost always means compounded product, and compounded product means no FDA review of potency or sterility. Read is compounded tirzepatide safe before you build a year-long protocol on a vial whose real concentration you have never verified.
Common Mistakes
Mistake 1: treating a starting dose as a maintenance dose. Zepbound's 2.5 mg is labelled as an initiation dose that is not intended for maintenance. Parking there for a year is an off-label decision made without a prescriber's input, and it forfeits the 15% to 21% weight loss the higher doses recorded. The fix: agree an escalation date with your prescriber, even if it is twelve weeks out rather than four.
Mistake 2: copying a microdose number across drugs. Tirzepatide at 1 mg produced 0.9 kg over 26 weeks. Retatrutide at 1 mg produced 8.7% body weight loss over 48 weeks. Same number, different molecule, ten-fold difference in outcome. The fix: check each drug's own dose-response arms, using the what is microdosing tirzepatide explainer for the tirzepatide numbers specifically.
Mistake 3: reconstituting once and never writing it down. Every dose error the FDA logged came from a mismatch between what was in the vial and what the person believed was in the vial. The fix: label the vial with mg/mL and the date, and confirm the unit conversion before every draw.
Mistake 4: blaming the drug when the dose was never therapeutic. People microdose for six months, lose 2 kg, and conclude GLP-1s do not work for them. They tested a dose no trial supports. The fix: reach a trial-tested dose with a prescriber before drawing conclusions about the molecule.
Frequently Asked Questions
What is microdosing GLP-1?
Microdosing means deliberately holding a GLP-1 dose below the range clinical trials tested, such as 0.1 mg of semaglutide weekly instead of 2.4 mg. It is off-label and unvalidated: no trial has measured weight loss at sub-therapeutic doses. Drug-specific numbers appear in the tirzepatide microdosing chart.
Does microdosing GLP-1 work for weight loss?
No trial has tested it, so the honest answer is that nobody knows. Dose-response data is discouraging: tirzepatide at 1 mg weekly produced 0.9 kg over 26 weeks against 11.3 kg at 15 mg. Sub-therapeutic doses sit on the shallow foot of the curve. See how to microdose semaglutide for what people report doing.
Is a starting dose the same as a microdose?
No. A 0.25 mg semaglutide start or a 2.5 mg tirzepatide start exists to let the gut adapt before escalation, and Zepbound's label states 2.5 mg is not for maintenance. Titration climbs; microdosing parks. Both use the same number for four weeks. Compare the semaglutide titration schedule.
Is there a GLP-1 microdosing chart I can follow?
No validated chart exists, because no trial has established a sub-therapeutic schedule for any GLP-1. Charts circulating online report what people do, not what works. The approved titration schedules are the only dosing tables with outcome data behind them. Run label doses through the semaglutide dosage calculator.
Does microdosing reduce GLP-1 side effects?
Lower doses generally produce fewer GI symptoms, but starting doses still cause nausea, which is precisely why titration schedules exist. A slower approved titration under a prescriber achieves the same tolerability while still reaching a therapeutic dose. Symptom rates across the class are in the GLP-1 side effect statistics.
Is microdosing a GLP-1 dangerous?
The direct pharmacological risk is low. The practical risks are real: hand-drawn doses from multi-dose vials caused overdoses of five to 20 times the intended amount in FDA adverse event reports, and stretched vials outlive their beyond-use date. Verify every conversion in the peptide unit converter.
Can I microdose to maintain weight loss after reaching my goal?
It is untested. The two withdrawal trials compared full dose against nothing, not against a reduced dose: stopping semaglutide caused 6.9% regain over 48 weeks and stopping tirzepatide caused roughly 14%. Whether a low dose holds weight is an open question. See the tirzepatide maintenance dose guidance.
Does microdosing save money?
Only if it works, and there is no evidence it does. A year at 1 mg of compounded tirzepatide costs roughly $3,000 to $4,800 and corresponds to the trial arm that lost 0.9 kg in 26 weeks. Price the outcome rather than the milligram using the peptide cost calculator.
The Bottom Line
Microdosing a GLP-1 means holding your dose below the range trials tested, and no trial has established that it produces meaningful weight loss. Tirzepatide at 1 mg weekly lost 0.9 kg over 26 weeks while 15 mg lost 11.3 kg. That gap is the whole argument.
Dose and response are not proportional. Below the therapeutic threshold you pay the full price, tolerate the side effects and sit on the shallow foot of the curve where the biology is happening and the scale does not move. Cost and nausea are legitimate reasons to want a smaller dose, and both have better answers: transparent pricing comparisons, and a slower approved titration run by a prescriber who has agreed a destination with you.
If you are working out doses, do it with real numbers rather than forum arithmetic. Use the tirzepatide dosage calculator and the retatrutide dosage calculator, and read the peptide safety guide before changing anything. Explore more evidence-based GLP-1 guides at peptidesexplorer.com, and take every dose decision to your prescriber.
Helpful Tools
Related Articles
Retatrutide Dosage: Titration Schedule
Retatrutide dosage chart with weekly titration schedule. Phase 2 & 3 trial data: up to 28.7% weight loss at 12 mg. Dose escalation and side effects.
Microdosing Tirzepatide Chart: Dose Guide
Microdosing tirzepatide chart with units, mg, and bac water conversions. Low-dose protocols for side effects, maintenance, and budget. Printable reference.
Semaglutide Mixing Chart: Every Vial Size (2026)
Semaglutide mixing chart for 3mg, 5mg, 10mg, 15mg vials. BAC water ratios, unit conversion, step-by-step reconstitution, titration schedule, and storage guide.
Microdosing Tirzepatide Explained
Microdosing tirzepatide means using 0.5-2.5 mg weekly instead of 5-15 mg. Protocols, clinical evidence, and side effect management.