You want to run tirzepatide at a lower dose than the standard 2.5 mg starting point, and you need the exact units to draw. Microdosing tirzepatide means using doses below the clinical minimum, typically 0.5 mg to 2 mg weekly, to reduce side effects, extend a vial, or maintain weight after reaching a goal. The chart below converts those microdoses into syringe units at the most common reconstitution ratios.
| Quick Reference | Details |
|---|---|
| Microdose range | 0.5 mg - 2 mg weekly |
| Standard starting dose | 2.5 mg weekly |
| Common reason | Side-effect control, maintenance, budget |
| Syringe type | U-100 insulin syringe |
| Key conversion | Units depend on reconstitution ratio |
| 1 mg at 10 mg/mL | 10 units |
| 0.5 mg at 10 mg/mL | 5 units |
| FDA status | Off-label dosing; not a labeled protocol |
Microdosing is not an FDA-approved protocol. Tirzepatide's label starts at 2.5 mg. This guide explains the conversions and the logic so you can dose accurately, but it is education, not medical advice. Always confirm your dose with a licensed provider.
For standard dosing, see our tirzepatide dosage chart in units. To understand the concept, read what is microdosing tirzepatide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
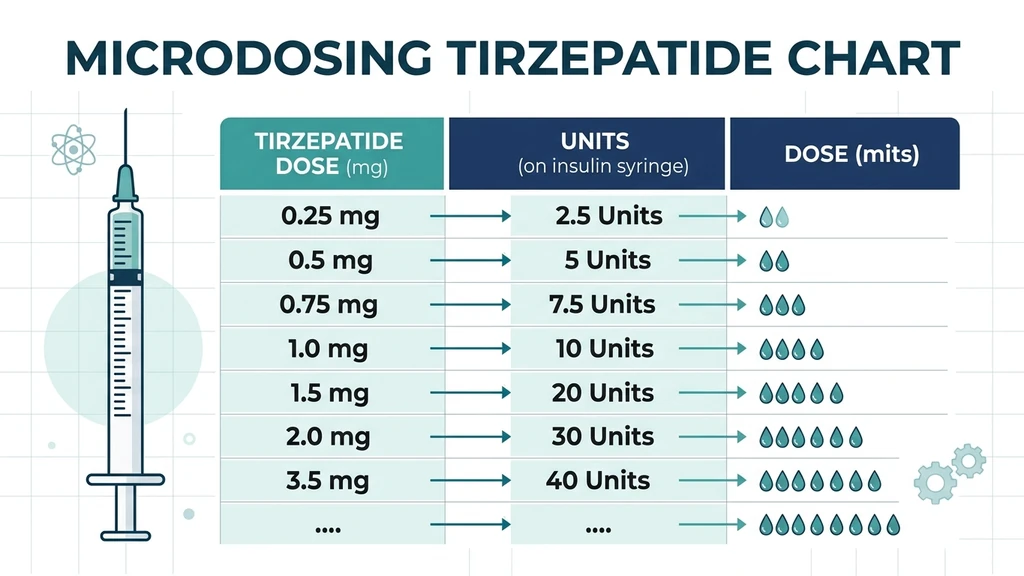
Microdosing Tirzepatide Chart: Units by Reconstitution
The single most important fact about reading any tirzepatide chart: units are meaningless without the reconstitution ratio. The same 1 mg dose can be 5 units or 20 units depending on how much bacteriostatic water you added. Always match your chart to your mixing ratio.
At 10 mg/mL (common: 10 mg vial + 1 mL bac water):
| Dose (mg) | Units (U-100) | Volume (mL) |
|---|---|---|
| 0.5 mg | 5 units | 0.05 mL |
| 0.75 mg | 7.5 units | 0.075 mL |
| 1 mg | 10 units | 0.10 mL |
| 1.5 mg | 15 units | 0.15 mL |
| 2 mg | 20 units | 0.20 mL |
At 5 mg/mL (10 mg vial + 2 mL bac water):
| Dose (mg) | Units (U-100) | Volume (mL) |
|---|---|---|
| 0.5 mg | 10 units | 0.10 mL |
| 0.75 mg | 15 units | 0.15 mL |
| 1 mg | 20 units | 0.20 mL |
| 1.5 mg | 30 units | 0.30 mL |
| 2 mg | 40 units | 0.40 mL |
Lower concentration means more units per dose, which makes small microdoses easier to measure accurately on a U-100 syringe. Use the peptide unit converter to check any ratio not listed here.
What Microdosing Tirzepatide Actually Means
Microdosing borrows a term from other fields, but here it has a specific meaning: dosing below the lowest labeled clinical dose. Tirzepatide's approved schedule begins at 2.5 mg weekly and titrates up to as high as 15 mg (Jastreboff et al., N Engl J Med, 2022). Anything under 2.5 mg is a microdose.
Think of it like seasoning food. The recipe calls for a full teaspoon, but some people are sensitive and prefer a pinch that still flavors the dish without overwhelming it. Microdosing tirzepatide aims for enough GLP-1 and GIP receptor activation to blunt appetite while staying under the threshold that triggers harsh nausea.
The trade-off is predictable. Lower doses mean fewer and milder side effects but slower or smaller weight loss. For some users, especially those maintaining a goal weight or extremely sensitive to GI effects, that trade is exactly what they want. For aggressive fat loss, microdosing underperforms standard titration.
Microdosing is an off-label practice. No clinical trial validated sub-2.5 mg dosing for efficacy. See what is microdosing tirzepatide for the full background.
Why People Microdose Tirzepatide
Four motivations drive almost every microdosing decision. Knowing which one applies to you shapes the right chart row to target.
Side-effect control. Nausea, constipation, and fatigue scale with dose. Users who cannot tolerate 2.5 mg sometimes start at 1 mg and climb slowly. See does tirzepatide cause constipation and does tirzepatide make you tired.
Maintenance after weight loss. After reaching a goal, many people drop to the smallest dose that prevents regain rather than stopping entirely. Our tirzepatide maintenance dose after weight loss guide covers this in depth.
Budget and vial stretching. A 10 mg vial used at 1 mg weekly lasts ten weeks instead of four. Microdosing cuts monthly cost substantially.
Sensitivity and small frames. Smaller or older users sometimes find standard doses too strong and prefer a gentler entry.
Each goal points to a different part of the chart. A maintenance user might sit at 1.5-2 mg, while someone purely controlling side effects on the way up might pause at 1 mg before escalating.
Microdosing Titration Schedule
If you microdose as a gentle on-ramp rather than a permanent protocol, a slow climb gives your gut time to adapt. This sample schedule is conservative and assumes a 10 mg/mL mix.
| Week | Dose | Units (10 mg/mL) | Goal |
|---|---|---|---|
| 1-2 | 0.5 mg | 5 units | Acclimate, assess tolerance |
| 3-4 | 1 mg | 10 units | Build appetite response |
| 5-6 | 1.5 mg | 15 units | Strengthen effect |
| 7-8 | 2 mg | 20 units | Approach standard floor |
| 9+ | 2.5 mg | 25 units | Enter labeled titration |
Hold at any step longer if side effects appear. There is no prize for rushing. The point of microdosing is comfort, and escalating before your gut adapts defeats the purpose.
Maintenance users run this in reverse, settling at the lowest dose that holds their weight. For the standard above-microdose schedule, see our tirzepatide dosage chart in units and the tirzepatide dosage calculator.
How to Measure a Microdose Accurately
The hardest part of microdosing is precision. A 5-unit dose leaves almost no margin for error on a standard syringe, and a small slip is a large percentage of the dose.
Use the right syringe. A U-100 insulin syringe with half-unit or single-unit markings is essential. The smaller the barrel (0.3 mL), the easier small doses are to read.
Dilute for easier measurement. Reconstituting at a lower concentration (5 mg/mL instead of 10 mg/mL) doubles the units per dose, spreading a tiny dose across more visible markings. A 0.5 mg dose at 5 mg/mL is 10 units instead of 5, which is far easier to draw accurately.
Draw at eye level. Hold the syringe vertically, tap out air bubbles, and read the plunger line straight on to avoid parallax error.
Reconstitute consistently. Use the same bac water volume every time so your chart stays valid. Changing the ratio mid-vial invalidates every unit conversion. See how to reconstitute tirzepatide and how much bacteriostatic water for semaglutide for the same mixing principles.
Accuracy matters more at microdoses than at standard doses, because the error is proportionally larger.
Microdosing vs Standard Dosing: The Trade-Off
Microdosing is not a free lunch. It buys tolerability at the cost of speed and, sometimes, total results.
| Factor | Microdose (0.5-2 mg) | Standard (2.5-15 mg) |
|---|---|---|
| Side effects | Minimal to mild | Moderate, dose-dependent |
| Weight loss speed | Slow | Faster |
| Monthly cost | Lower (vial lasts longer) | Higher |
| Appetite suppression | Modest | Strong |
| Best for | Maintenance, sensitivity, budget | Active fat loss |
| Evidence base | Off-label, no trials | FDA-approved, trial-backed |
The clinical weight-loss results everyone cites came from standard titration up to 10-15 mg, not microdoses (Jastreboff et al., N Engl J Med, 2022). If your goal is the dramatic loss seen in trials, microdosing will likely disappoint. If your goal is comfortable maintenance or a gentle start, it fits well.
Be honest about which camp you are in. Many people microdose hoping for full results with no side effects, then feel the protocol failed when it was never designed for that. See why am I not losing weight on tirzepatide if results stall.
Common Microdosing Mistakes
Mistake 1: Reading a units chart without checking the ratio. A chart built for 10 mg/mL is wrong if you mixed at 5 mg/mL. The fix: always match the chart to your exact reconstitution.
Mistake 2: Using a 1 mL syringe for tiny doses. Large-barrel syringes make 5-unit doses nearly impossible to read. The fix: use a 0.3 mL U-100 syringe.
Mistake 3: Expecting trial-level weight loss. Microdoses were never tested for the dramatic results seen at 10-15 mg. The fix: set realistic expectations or escalate to standard dosing.
Mistake 4: Changing the mixing ratio mid-vial. This silently invalidates every unit conversion you have memorized. The fix: reconstitute the same way every time.
Mistake 5: Microdosing to mask a quality problem. If a vial seems weak, microdosing will not fix underdosed or degraded product. The fix: verify your source and storage. See does tirzepatide expire and how long does tirzepatide last in the fridge.
Frequently Asked Questions
What is a microdose of tirzepatide?
Any weekly dose below the labeled 2.5 mg starting point, typically 0.5 mg to 2 mg. People microdose to limit side effects, maintain weight, or stretch a vial. It is an off-label practice with no clinical trial backing for efficacy. See what is microdosing tirzepatide for full context.
How many units is 1 mg of tirzepatide?
At a 10 mg/mL reconstitution (10 mg vial plus 1 mL bacteriostatic water), 1 mg is 10 units on a U-100 syringe. At 5 mg/mL it is 20 units. The unit count always depends on your mixing ratio. Confirm with our peptide unit converter.
How many units is 0.5 mg of tirzepatide?
At 10 mg/mL, 0.5 mg is 5 units. At 5 mg/mL it is 10 units. Because 5 units is hard to measure precisely, many microdosers reconstitute at a lower concentration to spread the dose across more visible syringe markings. See our tirzepatide dosage chart in units.
Does microdosing tirzepatide work for weight loss?
It can produce modest appetite suppression and slow weight loss, but it underperforms standard dosing. The dramatic results in clinical trials came from titration up to 10-15 mg, not microdoses. Microdosing suits maintenance and side-effect control better than aggressive fat loss. See tirzepatide maintenance dose after weight loss.
Can I microdose to avoid side effects?
Yes, this is one of the most common reasons. Nausea, constipation, and fatigue scale with dose, so starting at 0.5-1 mg and climbing slowly reduces them. Hold at each step until your gut adapts. See does tirzepatide cause constipation for managing GI effects.
What syringe should I use for microdosing?
A U-100 insulin syringe with a small 0.3 mL barrel and single or half-unit markings. The small barrel makes tiny doses easier to read accurately. Avoid 1 mL syringes for microdoses, as the markings are too coarse for precise measurement of 5-10 units.
Does microdosing save money?
Yes. A 10 mg vial used at 1 mg weekly lasts about ten weeks instead of four at standard dosing, cutting monthly cost significantly. This is a major reason people microdose. Use our peptide cost calculator to compare your cost per month at different doses.
The Bottom Line
A microdosing tirzepatide chart is only useful if it matches your reconstitution ratio. At 10 mg/mL, the core conversions are simple: 0.5 mg is 5 units, 1 mg is 10 units, 2 mg is 20 units. Mix at 5 mg/mL and every number doubles, which actually makes tiny doses easier to measure.
Microdosing trades speed for comfort. It shines for maintenance, side-effect control, sensitive users, and budget stretching, but it will not reproduce the dramatic trial results that came from full titration. Be clear about your goal before choosing a row on the chart.
Whatever dose you target, accuracy is everything at this scale. Use a fine U-100 syringe, reconstitute consistently, and confirm your conversions with the tirzepatide dosage calculator and peptide unit converter. For the full standard protocol, see our tirzepatide dosage chart in units, and always confirm your plan with a licensed provider.
Helpful Tools
Related Articles
Microdosing GLP-1: What It Is and the Risks
Microdosing GLP-1 means dosing below the range trials tested. What the dose-response data shows, how it differs from titration, and the cost and safety risks.
Microdosing Tirzepatide Explained
Microdosing tirzepatide means using 0.5-2.5 mg weekly instead of 5-15 mg. Protocols, clinical evidence, and side effect management.
Tirzepatide Maintenance Dose Guide
Most patients maintain on 5-10 mg tirzepatide weekly after reaching goal weight. SURMOUNT-4 data shows stopping leads to 50-67% weight regain within 12 months.
Retatrutide Dosage: Titration Schedule
Retatrutide dosage chart with weekly titration schedule. Phase 2 & 3 trial data: up to 28.7% weight loss at 12 mg. Dose escalation and side effects.