
You are over 40 and the changes are accelerating: skin losing firmness, joints aching in the morning, sleep disrupted by hormonal shifts. The top evidence-backed peptides for women over 40 are GHK-Cu (skin and collagen), collagen peptides (oral, for skin and joints), BPC-157 (recovery and gut health), CJC-1295/Ipamorelin (body composition), and PT-141 (libido, FDA-approved for women). Collagen production drops 30% within 5 years of menopause, and estrogen decline reshapes body composition, bone density, and mood (Brincat et al., Br J Obstet Gynaecol, 1987).
| Quick Reference | Details |
|---|---|
| #1 Skin/anti-aging | GHK-Cu |
| #1 Oral supplement | Collagen peptides (5-10g/day) |
| #1 Joint/gut recovery | BPC-157 |
| #1 Body composition | CJC-1295/Ipamorelin |
| #1 Libido (FDA-approved) | PT-141 / Vyleesi |
| Collagen loss rate | 30% in 5 years post-menopause |
| Key concern | Hormone-sensitive conditions |
| Blood work needed | Yes, including hormonal panel |
Use our peptide dosage calculator for personalized protocols. New to peptides? Start with our getting started guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Changes for Women After 40
The biological shifts after 40 are driven primarily by declining estrogen and progesterone. Perimenopause can begin as early as 38 and last a decade. The cascade touches nearly every system: skin, bones, metabolism, immune function, and neurological health.
Collagen Loss: 30% in 5 Years Post-Menopause
Estrogen is a direct regulator of collagen synthesis. When estrogen declines in perimenopause and drops sharply after menopause, skin collagen decreases by approximately 2.1% per year. Within 5 years of menopause, cumulative loss reaches 30% (Brincat et al., Br J Obstet Gynaecol, 1987).
The visible result: thinner skin, deeper wrinkles, loss of facial volume, and slower wound healing. Collagen loss also weakens tendons, ligaments, and joint cartilage. Peptides that stimulate collagen synthesis, whether topical GHK-Cu or oral collagen peptides, target this specific deficit.
Estrogen Decline and Perimenopause
Perimenopause begins 4-8 years before the final menstrual period. Estrogen levels fluctuate unpredictably during this phase, producing hot flashes, sleep disruption, mood changes, and irregular cycles. By menopause (defined as 12 consecutive months without a period), estrogen has dropped 60-80% from peak levels.
Peptides do not replace estrogen or hormone replacement therapy (HRT). They address downstream consequences: collagen loss, metabolic shifts, immune changes, and sexual function decline.
Bone Density Loss
Women lose bone density at approximately 1-2% per year in the decade after menopause. Estrogen is critical for osteoblast (bone-building cell) function. By age 60, one in three women has osteopenia or osteoporosis.
While no peptide directly replaces estrogen's bone-protective effects, GH-releasing peptides support IGF-1 levels that contribute to bone formation. Collagen peptides may improve bone mineral density markers in postmenopausal women in preliminary research.
Metabolic Shift and Body Composition
Estrogen decline redistributes fat from hips and thighs to the abdomen. Resting metabolic rate drops. Insulin sensitivity decreases. Women over 40 often report that the same diet and exercise regimen that maintained their weight at 35 no longer works.
GH-releasing peptides (CJC-1295/Ipamorelin) and metabolic peptides (MOTS-c) address the hormonal drivers of this shift. They work through IGF-1 and AMPK pathways, independent of estrogen.
Decreased Libido
Sexual desire declines in many women after 40, driven by falling testosterone (women produce testosterone too, just less of it) and estrogen. Hypoactive Sexual Desire Disorder (HSDD) affects approximately 10% of premenopausal women. PT-141 (bremelanotide, marketed as Vyleesi) is the only peptide FDA-approved specifically for this condition in women.
Top 8 Peptides for Women Over 40: Ranked
This ranking considers evidence quality, relevance to women-specific concerns after 40, safety in the perimenopausal and postmenopausal context, and accessibility (including oral options).
1. GHK-Cu: Skin, Collagen, and Anti-Aging
GHK-Cu is a naturally occurring tripeptide that modulates over 4,000 human genes, many involved in collagen synthesis, antioxidant defense, and tissue repair. In clinical studies, it reduced wrinkle volume by 55.8% and wrinkle depth by 32.8% over 12 weeks of topical application (Pickart et al., Int J Mol Sci, 2018).
For women over 40, GHK-Cu is the most directly relevant peptide. It targets the collagen deficit that drives visible skin aging and simultaneously supports scalp health and hair follicle function. Available as topical serums, subcutaneous injections, and microneedling solutions.
| GHK-Cu for Women 40+ | Details |
|---|---|
| Topical dose | 1-2% serum, applied twice daily |
| Injectable dose | 1-2 mg subcutaneous, daily |
| Key benefits | Collagen synthesis, wrinkle reduction, tissue repair |
| Results timeline | 4-8 weeks (topical); 8-12 weeks (injectable) |
| Side effects | Mild: skin redness (topical), injection site irritation |
Explore all delivery methods and dosing in our GHK-Cu benefits guide and GHK-Cu injection dosage guide.
2. Collagen Peptides: Oral Skin, Joint, and Bone Support
Oral collagen peptides (types I and III) are the most accessible peptide supplement for women over 40. Hydrolyzed collagen at 5-10g daily with vitamin C has demonstrated measurable improvements in skin elasticity (+15-20%), wrinkle depth reduction, and joint comfort in randomized controlled trials (Bolke et al., Nutrients, 2019).
A 2025 pilot study examined oral collagen peptides specifically for genitourinary syndrome of menopause and found improvements in vaginal mucosal health (PubMed 40507418). This is a unique application relevant to postmenopausal women that no other peptide addresses.
Take 5-10g hydrolyzed collagen with 500 mg vitamin C on an empty stomach. Results appear at 8-12 weeks for skin and 12-24 weeks for joints. No significant side effects at standard doses.
3. BPC-157: Joint and Gut Recovery
BPC-157 is derived from human gastric juice and promotes healing of tendons, ligaments, muscles, and gut lining. For women over 40, two applications stand out: joint recovery (addressing the collagen-weakened tendons and ligaments of perimenopause) and gut health (PMC12446177).
Gut permeability increases with age and hormonal changes. BPC-157 has demonstrated gastroprotective and gut-healing properties in animal models. Women experiencing IBS-like symptoms during perimenopause may benefit.
Standard dose: 250-500 mcg subcutaneous daily, or 500 mcg oral (capsule form, less studied). Inject near the affected joint for musculoskeletal issues, or in the abdominal area for gut applications. Cycle 4-8 weeks on, 2-4 weeks off. See our BPC-157 benefits for women.
4. CJC-1295 / Ipamorelin: Body Composition
The CJC-1295/Ipamorelin combination boosts growth hormone release, supporting lean mass retention and fat metabolism during the body composition shift that accompanies perimenopause. GH decline affects women similarly to men: less overnight repair, reduced fat oxidation, and slower recovery (PMC5632578).
Women typically use lower doses than men: 50-100 mcg of each peptide, subcutaneous before bed, 5 days per week. Monitor IGF-1 at baseline and 6 weeks. The primary benefits are improved sleep quality (within 2-4 weeks), gradual fat loss, and better recovery from exercise.
5. PT-141 / Bremelanotide: Libido (FDA-Approved for Women)
PT-141 (branded as Vyleesi) is the only peptide FDA-approved specifically for women. It treats HSDD (Hypoactive Sexual Desire Disorder) in premenopausal women by activating melanocortin-4 receptors in the brain, producing a dopamine-mediated increase in sexual desire (FDA Vyleesi Label, 2019).
In clinical trials, women receiving PT-141 reported significantly more satisfying sexual events and reduced distress related to low desire. The dose is 1.75 mg subcutaneous, self-administered at least 45 minutes before anticipated sexual activity. Maximum: 1 dose per 24 hours, 8 doses per month.
Side effects include nausea (40%), flushing (20%), and headache (11%). Nausea is most common with the first dose and diminishes with subsequent use. For dosing details, see our PT-141 dosage guide and peptides for libido overview.
6. Thymosin Alpha-1: Immune Support
Women over 40 experience immune changes beyond general immunosenescence. Autoimmune conditions are more prevalent in women, and the immune shifts of perimenopause can trigger flares or new onset autoimmune symptoms. Thymosin Alpha-1 (Ta1) modulates T-cell function and enhances immune surveillance without over-stimulating immune responses (Romani et al., Immunol Lett, 2007).
Standard dose: 1.6 mg subcutaneous, 2-3 times per week for 4-8 week courses. Women with autoimmune conditions should consult their rheumatologist before starting, as immune stimulation requires careful monitoring in this context.
7. MOTS-c: Metabolic Optimization
MOTS-c improves insulin sensitivity and glucose metabolism through AMPK activation. For women over 40 experiencing the metabolic slowdown of perimenopause, this addresses the cellular energy decline that makes weight management increasingly difficult (Lee et al., Cell Metab, 2015).
Dose: 5-10 mg subcutaneous, 3-5 times per week. Monitor fasting glucose at 4-week intervals. Coordinate with prescriber if taking diabetes medications or thyroid medications. Full protocol in our MOTS-c dosage guide.
8. KPV: Gut Health and Inflammation
KPV is a tripeptide derived from alpha-MSH with potent anti-inflammatory effects. It inhibits NF-kB signaling, reducing inflammatory cytokine production. For women over 40 dealing with increased gut inflammation, IBS symptoms, or inflammatory skin conditions, KPV offers targeted anti-inflammatory support.
KPV can be taken orally (capsule form, 200-500 mcg per day) or injected subcutaneously. Oral KPV reaches the gut lining directly, making it the preferred route for GI applications. Read our KPV peptide dosage guide and peptides for gut health overview.
Perimenopause vs Menopause: Different Peptide Approaches
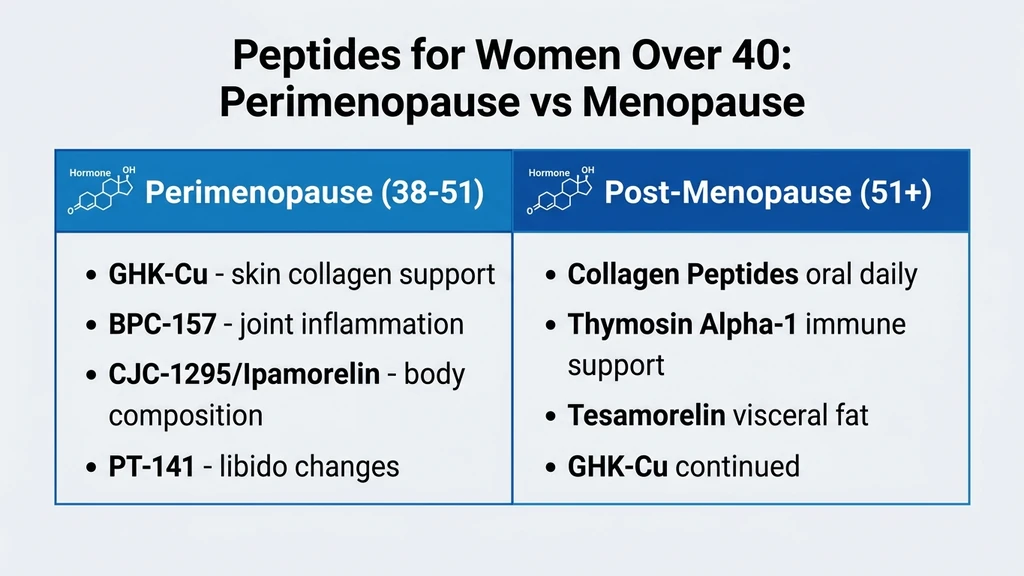
Perimenopause and post-menopause present different challenges. The peptide priorities shift as hormonal status changes.
| Factor | Perimenopause (40-50) | Post-Menopause (50+) |
|---|---|---|
| Estrogen status | Fluctuating, declining | Low, stable |
| Primary skin concern | Early collagen loss | Advanced collagen loss, thinning |
| Priority peptide | GHK-Cu (prevention) | GHK-Cu + Collagen peptides (repair) |
| Body composition | Fat redistribution starting | Visceral fat accumulation |
| GH peptide need | Moderate | Higher (GH decline steeper) |
| Libido | Variable decline | More consistent decline |
| PT-141 | FDA-approved for premenopausal HSDD | Off-label in postmenopausal women |
| Bone health concern | Moderate | High (1-2% loss/year) |
| Immune shifts | Autoimmune risk fluctuation | Immunosenescence |
| Gut health | IBS-like symptoms common | Continued gut permeability |
Women in perimenopause should focus on GHK-Cu, BPC-157, and body composition peptides. Post-menopausal women may add Thymosin Alpha-1 for immune support and increase collagen peptide dosing to 10g daily for bone and skin benefits.
Topical vs Injectable vs Oral Peptides for Women
Women over 40 have more delivery options than most peptide guides acknowledge. The choice depends on your primary goal, comfort with injections, and desired systemic versus local effects.
| Peptide | Topical | Injectable | Oral |
|---|---|---|---|
| GHK-Cu | 1-2% serum (skin-specific) | 1-2 mg SC (systemic) | Not available |
| Collagen peptides | Serums (limited absorption) | Not standard | 5-10g powder (best evidence) |
| BPC-157 | Not standard | 250-500 mcg SC (best absorption) | 500 mcg capsule (gut-specific) |
| CJC-1295/Ipamorelin | Not available | 50-100 mcg SC (only route) | Not available |
| PT-141 | Not available | 1.75 mg SC (FDA-approved route) | Not available |
| KPV | Not standard | 200-500 mcg SC | 200-500 mcg capsule (gut-specific) |
For skin-focused goals, start with topical GHK-Cu and oral collagen peptides. No needles required. For systemic benefits (body composition, recovery, libido), injection is the standard route.
Safety Considerations for Women Over 40
Women face unique safety considerations that men do not. Hormone-sensitive conditions, bone density, and breast health all factor into peptide selection and monitoring.
Hormone-Sensitive Conditions
GH-releasing peptides increase IGF-1, which can stimulate cell proliferation. Women with estrogen-receptor-positive breast cancer history, endometriosis, or uterine fibroids should consult their oncologist or gynecologist before starting GH peptides. This applies to CJC-1295, Ipamorelin, and Sermorelin.
GHK-Cu, collagen peptides, BPC-157, and KPV have no known hormone-stimulating effects and are generally considered safe in women with hormone-sensitive conditions, though data is limited.
Bone Density Monitoring
Women over 40 should have a baseline DEXA scan before starting peptide therapy, especially if postmenopausal. While GH peptides may support bone health indirectly through IGF-1, they are not a substitute for bisphosphonates or HRT in women with documented osteoporosis.
Repeat DEXA every 1-2 years. Oral collagen peptides at 10g daily may modestly support bone mineral density markers, though more research is needed.
Required Blood Work
Baseline labs for women over 40 before starting peptides:
- Estradiol, FSH, LH (hormonal status and menopausal staging)
- IGF-1 (baseline GH status)
- Complete metabolic panel (liver, kidney, glucose)
- Thyroid panel (TSH, free T3, free T4; thyroid issues are 5-8x more common in women)
- Fasting glucose + HbA1c
- Lipid panel
- CBC
- Vitamin D and ferritin (common deficiencies affecting peptide response)
- DEXA scan (bone density baseline, especially if postmenopausal)
Recheck IGF-1 at 6 weeks after starting GH peptides. Full monitoring in our peptide safety guide.
Frequently Asked Questions
What is the best peptide for women over 40?
GHK-Cu is the most versatile choice, addressing collagen loss, skin aging, and tissue repair through modulation of over 4,000 genes. For an oral option requiring no injections, hydrolyzed collagen peptides at 5-10g daily show significant skin and joint improvements within 8-12 weeks in clinical trials.
Is PT-141 safe for women?
PT-141 (bremelanotide, marketed as Vyleesi) is the only peptide FDA-approved specifically for women, indicated for HSDD in premenopausal women. The dose is 1.75 mg subcutaneous. Side effects include nausea (40%) and flushing (20%). It addresses desire through brain melanocortin receptors, not hormonal pathways.
Can peptides help with menopause symptoms?
Peptides address several menopause-related concerns: collagen loss (GHK-Cu, collagen peptides), body composition changes (CJC-1295/Ipamorelin), joint pain (BPC-157), decreased libido (PT-141), and gut inflammation (KPV). They do not replace hormone replacement therapy and do not directly treat hot flashes or mood symptoms.
Are peptides safe during perimenopause?
Most peptides are safe during perimenopause with appropriate monitoring. GHK-Cu, collagen peptides, BPC-157, and KPV have no known hormone-stimulating effects. GH-releasing peptides require IGF-1 monitoring. Women with hormone-sensitive conditions should consult their gynecologist before starting any peptide protocol.
Do I need injections for peptides to work?
No. Oral collagen peptides (5-10g daily) have strong clinical evidence for skin and joint benefits. Topical GHK-Cu (1-2% serum) works for skin applications. Oral KPV and BPC-157 capsules exist for gut-specific targets. Injectable peptides offer systemic effects but are not the only option.
How much collagen should women over 40 take daily?
Clinical trials showing skin and joint benefits used 5-10g of hydrolyzed collagen peptides (types I and III) daily. Take on an empty stomach with 500 mg vitamin C, which is required for collagen synthesis. Results appear at 8-12 weeks for skin elasticity and 12-24 weeks for joint improvement.
Can peptides help with perimenopause weight gain?
CJC-1295/Ipamorelin supports GH-mediated fat metabolism and lean mass retention. MOTS-c improves insulin sensitivity. Neither replaces dietary and exercise changes, but they address the hormonal drivers that make weight management harder after 40. Women typically start at 50-100 mcg of CJC-1295/Ipamorelin.
Should I use peptides or HRT?
Peptides and HRT address different problems. HRT replaces estrogen and progesterone, treating hot flashes, bone loss, and vaginal dryness directly. Peptides target collagen synthesis, GH decline, tissue repair, and libido through non-hormonal pathways. Many women use both. Discuss with your gynecologist or endocrinologist.
The Bottom Line
Women over 40 face collagen loss, metabolic shifts, immune changes, and hormonal fluctuations that peptides can partially address. GHK-Cu targets the collagen deficit driving visible skin aging. Oral collagen peptides provide the most accessible supplementation with clinical evidence for skin and joints. BPC-157 supports joint recovery and gut health. PT-141 is the only FDA-approved peptide for female sexual dysfunction.
Start simple. Topical GHK-Cu and oral collagen require no injections and no blood work for healthy women. If you choose injectable peptides, get baseline labs including estradiol, IGF-1, thyroid panel, and a metabolic panel. Monitor every 3-6 months.
Use our peptide dosage calculator for personalized protocols. For men-specific approaches, see our peptides for men over 40 and peptides for men over 50 guides. Review our peptide safety guide before starting. Consult your physician, especially if you have a history of hormone-sensitive conditions.
Helpful Tools
Related Articles
Best Peptides for Men Over 40: Ranked Guide (2026)
Top 10 peptides for men over 40: CJC-1295, BPC-157, PT-141, Tesamorelin ranked by evidence. Stacking protocols, dosing, and safety monitoring guide.
Best Peptides for Men Over 50: Protocols
Top 8 peptides for men over 50 ranked by safety. Sermorelin, BPC-157, Tesamorelin protocols with adjusted dosing and blood work requirements.
Thymosin Alpha-1 Benefits Guide
Thymosin Alpha-1 (Ta1) benefits backed by clinical trials: immune support, cancer adjunct therapy, vaccine enhancement, and anti-aging. Dosage and safety.
What Do Peptides Do for Skin? Benefits & Types
Peptides boost collagen by up to 65%, reduce wrinkles, and strengthen the skin barrier. Which types work, how to use them, and clinical evidence.