You have a reconstituted vial of MOTS-c in the fridge and a loaded insulin syringe. Inject MOTS-c subcutaneously into the fatty tissue of the abdomen, at least 2 inches (5 cm) away from the navel. The outer thigh and the "love handles" (flanks) are equally valid sites. Pinch the fat, insert the needle at a 45 to 90 degree angle, and deliver into the subcutaneous layer, never into muscle.
MOTS-c is studied almost exclusively by subcutaneous injection in animal models, where the peptide signals through the AMPK pathway after entering circulation (Reynolds et al., 2021). The abdomen is the default site because it holds the largest, most consistent fat pad and is easy to pinch with one hand.
MOTS-c is a research peptide. No form is approved by the FDA for human use. Consult a healthcare provider before injecting anything. For amounts and frequency, see the MOTS-c dosage guide; for mixing the vial, see how to reconstitute MOTS-c.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
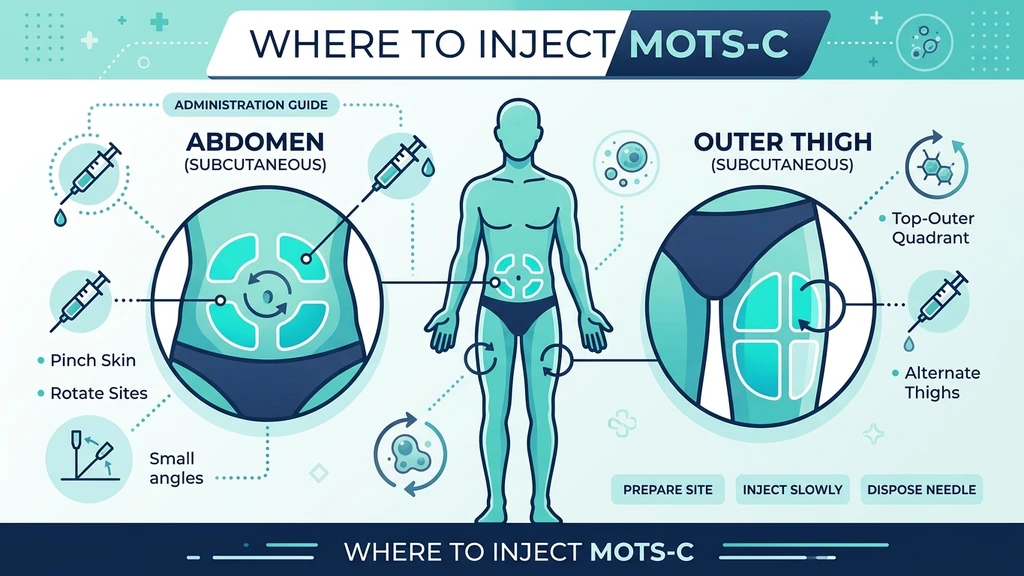
Best Injection Sites for MOTS-c
MOTS-c works systemically. Once it reaches the bloodstream from the subcutaneous fat, it travels to skeletal muscle and other tissues regardless of which site you chose. That means the "best" site is whichever one has enough fat to pinch, rotates easily, and stays out of your way during exercise.
Three sites cover nearly every protocol: the abdomen, the outer thigh, and the flanks. Each has a fold of subcutaneous fat sitting over a layer that contains few large blood vessels and nerves, which keeps bruising and pain low.
| Site | Where Exactly | Pros |
|---|---|---|
| Abdomen | 2+ inches (5 cm) from the navel, below the ribs, above the hip crease | Largest fat pad, easiest one-hand pinch, most consistent absorption |
| Outer thigh | Front-outer quadrant, a hand's width above the knee and below the hip | Easy to see, large rotation area, good for self-injection while seated |
| Flanks (love handles) | The fatty roll at the side of the waist | Generous fat, far from muscle, comfortable angle |
| Back of upper arm | Triceps fat pad, rear of the arm | Useful for rotation; usually needs a second person to pinch |
The abdomen is the first choice for most people. Keep a clear 2-inch (5 cm) radius around the navel, where tissue is thinner and absorption is less predictable. Avoid scars, moles, stretch marks, bruises, and any lump or hardened patch.
Because MOTS-c does not act locally on a single joint or muscle the way some healing peptides do, you do not need to inject "near" a target area. Pick whichever fatty site is convenient, then rotate.
Subcutaneous vs. Intramuscular for MOTS-c
Subcutaneous (under the skin, into fat) is the standard route for MOTS-c. Published research administers MOTS-c subcutaneously or by intraperitoneal injection in animals, and the subcutaneous route translates most directly to human research protocols (Reynolds et al., 2021).
Intramuscular injection (into the muscle belly) is unnecessary for MOTS-c and adds risk. IM injections use longer needles, hurt more, bruise more often, and reach blood vessels more easily. They offer no proven advantage because MOTS-c needs to enter the bloodstream, not sit inside one specific muscle.
Subcutaneous delivery uses a short, fine needle (typically a 29 to 31 gauge, 1/2 inch insulin syringe), produces a slower and steadier release from the fat, and is far simpler to perform on yourself. Unless a knowledgeable clinician directs otherwise, keep MOTS-c subcutaneous. For broader injection mechanics shared across peptides, see how to inject peptides.
Step-by-Step Injection Technique
Clean technique matters more than the exact site. Most injection problems trace back to a skipped step, not a wrong location.
- 1.Wash and gather. Wash your hands. Lay out the reconstituted vial, an insulin syringe, two alcohol swabs, and a sharps container. Most MOTS-c users draw a small volume with a 29 to 31 gauge, 1/2 inch (12.7 mm) insulin syringe.
- 2.Swab the vial. Wipe the rubber stopper with one alcohol swab and let it dry for a few seconds.
- 3.Draw the dose. Pull air into the syringe equal to your dose, inject it into the vial, then invert and draw your measured volume. Confirm the amount against your reconstitution calculator. Flick out air bubbles and push them back into the vial.
- 4.Prep the skin. Wipe the chosen site with the second swab. Let it dry fully so the alcohol does not sting on entry.
- 5.Pinch and insert. Pinch a fold of fat between thumb and forefinger. Insert the needle in one smooth motion at 45 to 90 degrees. Use 90 degrees if you have a generous pinch; use 45 degrees if you are lean.
- 6.Inject and withdraw. Press the plunger steadily over a few seconds. Withdraw the needle at the same angle, release the pinch, and apply light pressure with a clean swab. Do not rub.
- 7.Dispose. Drop the syringe into the sharps container immediately. Never recap with two hands.
If you see more than a drop of blood or feel a sharp deep ache, you likely went too deep or nicked a small vessel. Apply pressure and choose a fresh spot for the next dose.
Site Rotation to Avoid Lipohypertrophy and Bruising
Repeated injections into one spot cause lipohypertrophy, firm fatty lumps that form when tissue is traumatized over and over. Beyond the cosmetic bump, lipohypertrophy slows and scrambles absorption, so the peptide no longer reaches the bloodstream predictably (Frid et al., 2016).
Rotation is the fix. Keep each injection at least 1 inch (2.5 cm) from your last one, and divide each site into a grid you work through in order. A simple system: split the abdomen into four quadrants, and treat each thigh and flank as its own zone.
- Within a session: if you inject more than once, separate the spots by at least 1 inch (2.5 cm).
- Across days: move to a new quadrant or a different site each time rather than returning to yesterday's spot.
- Across weeks: cycle through abdomen, thigh, and flank so no single area absorbs every dose.
To limit bruising, avoid visible veins, let the alcohol dry before insertion, insert and withdraw at the same angle, and press (never rub) afterward. If a spot turns hard, lumpy, red, or sore, retire it from the rotation until it fully heals, which can take weeks.
Timing: Fasted, Morning, or Pre-Exercise
MOTS-c is often described as an "exercise mimetic" because it activates AMPK, the same metabolic switch that exercise flips (Reynolds et al., 2021). That biology is why many users time their injection to morning or to a workout.
A common research-informed pattern is to inject in the morning, often fasted, when the metabolic signaling overlaps with the body's natural circadian rhythm. Others inject 30 to 60 minutes before training, reasoning that the peptide and the exercise stimulus reinforce each other.
Timing does not change *where* you inject. The site stays subcutaneous fat regardless of clock. What timing interacts with is dose and frequency: most protocols use a few injections per week rather than daily, so the day you inject matters more than the hour. Pick a consistent window you can repeat, then hold it. For amounts and weekly frequency, see the MOTS-c dosage guide, and for total program duration see MOTS-c cycle length.
Common Injection Mistakes
Most MOTS-c injection problems are avoidable and come from a short list of repeated errors.
- Injecting too close to the navel. Tissue within 2 inches (5 cm) of the navel is thinner and absorbs unevenly. Stay outside that radius.
- Going intramuscular by accident. Using a long needle or skipping the pinch on lean tissue drives the dose into muscle. Pinch the fat and use a 1/2 inch insulin needle.
- Reusing one spot. Hitting the same site repeatedly builds lipohypertrophy and ruins absorption. Rotate every dose.
- Injecting through alcohol. Pushing the needle in while the swab is still wet causes stinging and irritation. Let the skin dry.
- Rubbing the site. Rubbing after withdrawal spreads the depot and increases bruising. Apply gentle pressure instead.
- Skipping the air bubble check. Large air bubbles throw off your measured dose. Flick them out before injecting.
- Wrong storage between doses. Reconstituted MOTS-c is fragile and should stay refrigerated. Storage errors degrade potency before the needle ever touches skin.
For the wider safety picture, including sterility and handling, read the peptide safety guide, and review possible reactions in MOTS-c side effects.
Frequently Asked Questions
Where is the best place to inject MOTS-c?
The abdomen is the best place for most people, at least 2 inches (5 cm) from the navel, because it holds a large fat pad that is easy to pinch with one hand. The outer thigh and flanks work just as well. See full site details in this MOTS-c injection guide.
Is MOTS-c injected subcutaneous or intramuscular?
MOTS-c is injected subcutaneously, into the fat under the skin, in nearly all research protocols. Intramuscular injection adds pain and bruising risk with no proven benefit, since MOTS-c acts after entering the bloodstream. General technique applies; see how to inject peptides.
What needle size should I use for MOTS-c?
A standard insulin syringe with a 29 to 31 gauge, 1/2 inch (12.7 mm) needle is appropriate for subcutaneous MOTS-c. The thin gauge minimizes pain and the short length keeps the dose in fat rather than muscle. Confirm your draw volume with the reconstitution calculator.
How do I rotate MOTS-c injection sites?
Keep each injection at least 1 inch (2.5 cm) from the last, and divide the abdomen into quadrants while treating each thigh and flank as its own zone. Rotate through them so no area gets every dose. This prevents lipohypertrophy, as covered in where to inject GHK-Cu.
Does MOTS-c injection hurt or bruise?
Subcutaneous MOTS-c injection is usually nearly painless with a fine insulin needle. Bruising happens when you nick a small vessel or rub the site afterward. Let alcohol dry, avoid visible veins, and apply gentle pressure. Possible reactions are detailed in MOTS-c side effects.
When should I inject MOTS-c, morning or before exercise?
Many users inject in the morning, often fasted, or 30 to 60 minutes before training, because MOTS-c activates the same AMPK pathway as exercise. Timing affects metabolic overlap, not the injection site. Pick a consistent window and review frequency in the MOTS-c dosage guide.
Can I inject MOTS-c in the same spot as BPC-157?
You can use the same general regions, like the abdomen, but place each peptide at least 1 inch (2.5 cm) apart and rotate both. Unlike BPC-157, MOTS-c does not need to be injected near a target area. See site logic in where to inject BPC-157.
The Bottom Line
MOTS-c goes subcutaneously into fat: the abdomen (2+ inches from the navel), the outer thigh, or the flanks. Use a 29 to 31 gauge, 1/2 inch insulin needle, pinch the fat, inject at 45 to 90 degrees, and rotate at least 1 inch each time to keep absorption consistent and lumps away. Clean technique and disciplined rotation matter more than the exact spot.
MOTS-c remains a research peptide with no FDA-approved human use, and the human evidence base is thin. Treat every protocol as experimental and discuss it with a qualified healthcare provider before starting. To plan your protocol end to end, pair this guide with the MOTS-c dosage guide, how to reconstitute MOTS-c, and real-world expectations in MOTS-c before and after. Explore more peptide guides and tools at PeptidesExplorer.com.
Helpful Tools
Related Articles
MOTS-c Before and After: Results & Timeline
See realistic MOTS-c before and after results, a week-by-week timeline, what the research shows, and the factors that decide whether you respond.
How to Reconstitute MOTS-c: Step-by-Step
How to reconstitute MOTS-c step by step. Mixing table for 5mg and 10mg vials, syringe unit math, storage shelf life, and the reconstitution mistakes to avoid.
Glutathione Peptide: Is It Actually a Peptide?
Glutathione is a genuine tripeptide with an unusual gamma bond. What bioavailability trials actually found, why IV skin lightening is risky, and what works.
Kisspeptin Peptide: What the Human Evidence Shows
Kisspeptin peptide sits upstream of GnRH and drives LH, FSH, and testosterone. Human trial doses, kisspeptin-10 vs 54, and the desensitization risk.