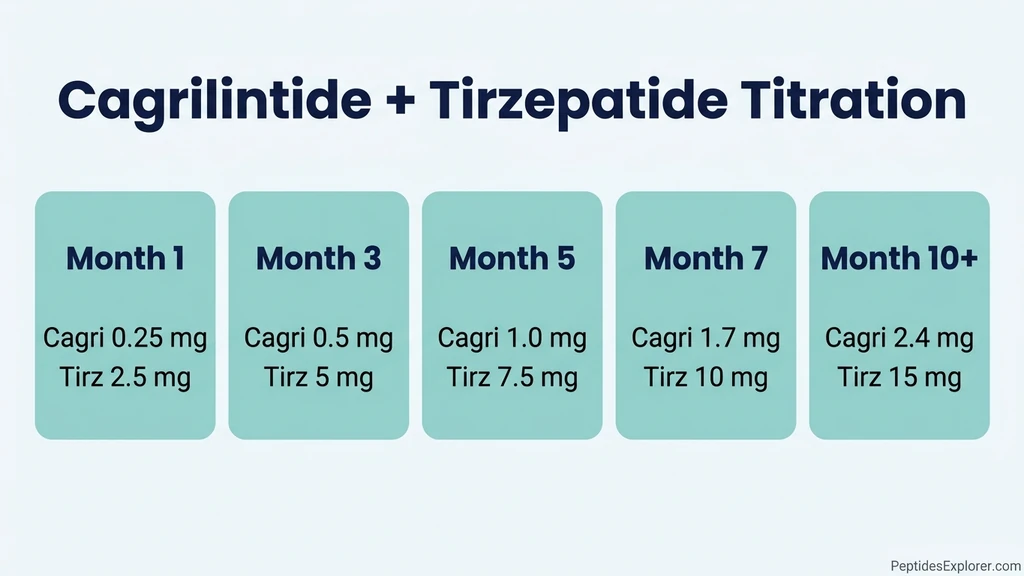
You are looking at two vials on the counter: cagrilintide and tirzepatide. Your provider sent you home with a sticky note that says "0.5 mg cagri + 5 mg tirz weekly, same day." Two separate syringes, two separate sites, one weekly ritual. The standard compounded protocol runs cagrilintide from 0.25 mg up to 2.4 mg per week, paired with tirzepatide from 2.5 mg up to 15 mg per week. You inject both on the same day in different spots, you bump the dose every 4 weeks, and you never raise both drugs in the same week. This combo is not FDA-approved. The only published human trial data comes from CagriSema (cagrilintide + semaglutide, a different drug), and no Phase 3 study has tested cagri + tirz together. Everything below comes from compounding-pharmacy protocols and adjacent trials, not from controlled evidence.
| Quick Reference | Detail |
|---|---|
| FDA approval status | Not approved as a combination |
| Published human trial data | None for this combination (CagriSema = cagri + semaglutide, separate drug) |
| Cagrilintide dose range | 0.25 to 2.4 mg/week |
| Tirzepatide dose range | 2.5 to 15 mg/week |
| Injection frequency | Both weekly, same day, separate injections |
| Titration interval | 4 weeks per step |
| Rule | Never escalate both drugs in the same week |
| Primary side effect | Cumulative GI (nausea 30-50%, diarrhea 20-30%) |
| Origin | Extrapolated from CagriSema protocols + tirzepatide monotherapy |
Here is what is happening inside you. Amylin is the satiety hormone your pancreas releases after a meal. Cagrilintide is a long-lasting copy of it. It tells your brain you are full, even when you have not eaten. Tirzepatide hits two satiety receptors at once: GLP-1 (slows your stomach emptying so meals last longer in your gut) and GIP (helps fat cells respond better to insulin).
It is like pulling three different brakes on hunger at once: pancreas (amylin), gut (GLP-1), fat cells (GIP). Each works differently. Stacking them is supposed to add up, but so do the side effects. For the cagrilintide-only side of this picture, see cagrilintide weight loss dosage.
This is educational content. Talk to your provider before combining any medications.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Your Provider Stacked These Two
Cagrilintide and tirzepatide both treat obesity, and they hit different receptors. Your provider is betting on a triple-mechanism idea. If semaglutide + cagrilintide (CagriSema) produced 20.4% weight loss in the REDEFINE 1 trial over 68 weeks (Garvey et al., 2025), then swapping in tirzepatide should in theory match or beat it. Tirzepatide alone reached 20.9% weight loss at the 15 mg dose in SURMOUNT-1 (Jastreboff et al., 2022).
Here is the mechanism map in plain terms. Cagrilintide is a long-acting amylin copy. Engineers attached a fatty acid chain so it sticks to your blood albumin and lasts a full week (Kruse et al., 2021). It quiets glucagon, slows your stomach, and tells your hypothalamus that you are full.
Tirzepatide is the dual-receptor drug. The GLP-1 side slows your gastric emptying and pushes insulin when you eat. The GIP side improves how your fat cells handle insulin and may soften the nausea you would get from GLP-1 alone.
No Phase 3 trial has tested cagri + tirz head-to-head. The closest data is REDEFINE 1 (cagri + sema) and SURMOUNT-1 (tirz alone). Anyone who sells you this stack is extrapolating.
Some compounding pharmacies offer both drugs and market a co-administration protocol. This is a regulatory grey zone. Tirzepatide is FDA-approved and patented by Eli Lilly. Cagrilintide had its NDA filed in December 2025 and is still unapproved. For the legal context, see FDA peptide crackdown and are peptides legal.
Your Standard Titration Protocol (Compounded)
The most common compounded protocol stacks both injections on the same day, raises one drug per month, and holds at maintenance once you find the dose your gut tolerates.
| Month | Cagrilintide weekly | Tirzepatide weekly | Notes |
|---|---|---|---|
| 1 | 0.25 mg | 2.5 mg | Starter. Both drugs at the lowest dose. |
| 2 | 0.25 mg | 5 mg | Tirzepatide bumps to 5 mg. Hold cagri. |
| 3 | 0.50 mg | 5 mg | Cagri bumps. Hold tirz. |
| 4 | 0.50 mg | 7.5 mg | Tirz bumps. Hold cagri. |
| 5 | 1.0 mg | 7.5 mg | Cagri bumps. Hold tirz. |
| 6 | 1.0 mg | 10 mg | Tirz bumps. Hold cagri. |
| 7 | 1.7 mg | 10 mg | Cagri approaches target. |
| 8 | 1.7 mg | 12.5 mg | Tirz approaches target. |
| 9 | 2.4 mg | 12.5 mg | Cagri at target. |
| 10+ | 2.4 mg | 15 mg | Both at target, or stop one step below if your gut says no. |
The core rule: never escalate both drugs in the same week. Bump cagri from 0.5 to 1.0 mg AND tirz from 5 to 7.5 mg in the same week, and you have effectively doubled hunger suppression overnight. Expect 2 to 3 days of brutal nausea, possible vomiting, and a real risk of dehydration that lands people in the ER. Spacing the bumps by a month gives your body time to settle.
Slower is always safer. If a dose level gives you 5 to 7 days of nausea, hold for an extra 4 weeks before the next step. The CagriSema trial logged 79.6% GI side effects at similar levels with cagri + sema. Tirzepatide alone already runs 30 to 50% nausea, so cagri + tirz likely lands in the 60 to 80% range during titration.
Injection day looks like this: both drugs are subcutaneous, both are weekly. Use two separate syringes and two separate sites. Left abdomen for one, right thigh for the other works fine. Never mix them in the same syringe. See best injection sites for tirzepatide and the tirzepatide dosage calculator for site rotation guidance.
How Your Stack Differs From CagriSema
CagriSema is Novo Nordisk's investigational drug. It is cagrilintide and semaglutide co-formulated in one vial, one weekly injection. Your cagri + tirzepatide stack is two separate drugs, two separate shots, no FDA approval.
| Attribute | CagriSema (cagri + sema) | Cagri + Tirz stack |
|---|---|---|
| Approval status | NDA filed Dec 2025 | None |
| Formulation | Single co-formulated vial | Two separate drugs |
| Mechanism | Amylin + GLP-1 | Amylin + GLP-1 + GIP |
| Trial data | REDEFINE 1 (22.7% WL at 68 weeks) | None published |
| Weekly injection | One shot | Two shots |
| Evidence strength | Phase 3 completed | Anecdotal |
The GIP angle is the big "maybe" of your stack. Tirzepatide's GIP receptor activation is one reason it beat semaglutide in head-to-head data (22.5% vs 14.9% mean weight loss). If that GIP effect adds to cagrilintide's amylin effect, your stack could in theory beat CagriSema. That is speculation until a real trial runs.
The flip side is also real. Side effects from GLP-1, GIP, and amylin all converge on similar gut pathways. Nausea does not stack neatly. A 30% nausea rate from tirz plus a 40% rate from cagri is not 70%. The combined rate often pushes past 80% at peak titration, which is when most people quit. CagriSema's co-formulation at lower effective doses may be friendlier to your stomach than your two-shot stack.
For the cagrilintide monotherapy and CagriSema data, see cagrilintide weight loss dosage. For tirzepatide alone, see how to inject tirzepatide and tirzepatide dosage chart in units. For the survodutide alternative that uses a triple-receptor design natively, see survodutide vs tirzepatide.
What Your Side Effects Will Look Like
The cumulative gut burden is the main reason to think twice about this stack. You should know what to expect on injection day and the days after.
What you can expect (extrapolated from CagriSema + tirzepatide data): - Nausea: 40 to 60% during titration weeks, dropping to 10 to 20% once you settle at maintenance - Diarrhea: 20 to 30% at peak dose levels - Constipation: 15 to 25%, often alternating with diarrhea - Vomiting: 10 to 20% during dose increases - Injection site reactions: 5 to 10% per site - Pancreatitis: rare, same risk as either drug alone, not clearly worse together - Thyroid C-cell tumor risk: tirzepatide's boxed warning still applies
Stop the stack and call your provider for any of these: - Severe abdominal pain that does not let up (rule out pancreatitis) - Vomiting that lasts more than 48 hours - Signs of dehydration: dark urine, dizziness on standing, headache - A new lump in your neck or trouble swallowing (thyroid pathology) - New mood changes or suicidal thoughts (both drugs carry this warning)
If you cannot tolerate the next titration step, drop one level, hold for 4 more weeks, and try again. Do not skip a maintenance dose of either drug. Miss your cagrilintide for more than 10 days and you essentially restart the titration clock for that drug. Tirzepatide has a 5-day half-life and is more forgiving.
Drug interactions: both drugs slow your stomach, which can wreck the absorption of any oral medication you take within 2 hours of injection. This matters most for oral contraceptives, thyroid meds, and warfarin. See tirzepatide drug interactions for the full list that applies here.
For the broader safety picture on GLP-1 stacking, see can tirzepatide cause anxiety and tirzepatide long-term side effects.
When This Stack Makes Sense (And When It Does Not)
You are a reasonable candidate if: - You have plateaued on tirzepatide alone at 15 mg for 6+ months and still have significant weight to lose - You are working with a specialist who knows this is unapproved - You are willing to titrate slower than either drug alone would require
You are a poor candidate if: - You are starting your first GLP-1 (start with tirzepatide or semaglutide alone first) - Your BMI is under 30 with no metabolic issues (the risk does not justify a triple-agent stack) - You have a history of pancreatitis, medullary thyroid carcinoma, or MEN-2 syndrome (both drugs are contraindicated) - You are pregnant, breastfeeding, or planning conception within 2 months (both drugs are contraindicated) - You found this stack on social media and called it "next level". Marketing is not evidence
What this stack will not do for you: - Speed up weight loss past what tirzepatide alone produces (unproven) - Reduce side effects compared to either drug alone (it adds them) - Replace protein, resistance training, and sleep - Work without consistent weekly dosing
If your real problem is plateau, fix the protocol you have first. The usual culprits: protein under 1.6 g/kg lean mass, no resistance training, fewer than 7 hours of sleep, and hidden calorie sources you stopped tracking. See why am I not losing weight on tirzepatide for the full plateau checklist before you add a second drug.
Frequently Asked Questions
Is cagrilintide + tirzepatide FDA-approved?
No. Neither drug is approved for use in combination. Tirzepatide is FDA-approved alone (Mounjaro, Zepbound). Cagrilintide had its NDA filed in December 2025 as part of CagriSema (cagri + semaglutide); it has no standalone approval. Your cagri + tirz combo is compounded only, with no Phase 3 data behind it. See cagrilintide weight loss dosage for the approval timeline.
What is the typical dose of cagrilintide when stacked with tirzepatide?
You start at 0.25 mg weekly and titrate up every 4 weeks through 0.5, 1.0, 1.7, and 2.4 mg as your gut allows. The target maintenance dose is 2.4 mg weekly, matching the CagriSema trial protocol. Never raise cagrilintide in the same week you raise tirzepatide. The side effects stack and you will pay for it. See cagrilintide weight loss dosage for the full schedule.
Can I mix cagrilintide and tirzepatide in the same syringe?
No. Use two separate syringes and two separate injection sites on the same day. Mixing can destabilize either peptide and changes how fast each one absorbs. Standard practice is two abdominal injections at least 2 inches apart, or one in your abdomen and one in your thigh. See best injection sites for tirzepatide.
Will stacking cagrilintide with tirzepatide produce more weight loss than tirzepatide alone?
Unknown. No controlled trial has tested this. The CagriSema trial (cagri + sema) produced 22.7% weight loss at 68 weeks vs 14.9% for semaglutide alone. If the same additive logic applies to tirzepatide (22.5% alone), your stack could in theory reach 25 to 30% weight loss. That is extrapolation. For published data, see cagrilintide weight loss dosage and retatrutide vs tirzepatide for alternative triple-mechanism drugs.
What side effects should I expect with the cagri + tirz stack?
Plan on nausea (40 to 60% during titration), diarrhea (20 to 30%), constipation (15 to 25%), and vomiting (10 to 20%). Side effects peak when you raise a dose and settle at maintenance. Combined GI rates are higher than either drug alone. See tirzepatide long-term side effects and can tirzepatide cause anxiety for the single-drug baselines.
How is this different from CagriSema?
CagriSema is cagrilintide + semaglutide co-formulated in one injection, with Phase 3 data and an NDA filed. Your cagri + tirzepatide stack is compounded from two separate drugs, with no Phase 3 data. The triple-agonist advantage of cagri + tirz (the added GIP mechanism) is theoretical until a trial tests it. For CagriSema specifics, see cagrilintide weight loss dosage.
Do I need higher doses of either drug when stacking?
No. Use the standard titration for each drug (cagrilintide to 2.4 mg, tirzepatide to 10 to 15 mg). Higher doses do not give you proportional benefit and they ramp up your side effects. If 2.4 mg cagri + 15 mg tirz does not move the scale, a different mechanism class like retatrutide is more useful than pushing the dose. See retatrutide dosage.
What should I do if I cannot tolerate the stack?
Drop back to the previous tolerated dose level and hold for 4 weeks before retrying the bump. If you still cannot tolerate it, stop cagrilintide and continue tirzepatide alone. Tirzepatide is the primary effective drug; cagrilintide is the addition. Dropping the addition is always better than dropping both. For reintroduction protocols after a stop, see how to inject tirzepatide.
The Bottom Line
Cagrilintide + tirzepatide is an unapproved combination with no Phase 3 trial data. The dosing protocols floating around compounding-pharmacy communities are extrapolated from CagriSema (which uses semaglutide, not tirzepatide) and from tirzepatide alone. The triple-mechanism story is theoretically sound: amylin + GLP-1 + GIP pulls three independent brakes on appetite. Whether that translates to better outcomes than tirzepatide alone is still unknown.
If you and your prescriber decide to run this stack, the rules are simple. Bump one drug per 4-week window, never both. Use separate injection sites. Expect cumulative GI side effects, especially during the first 4 to 6 months. If your gut taps out, drop cagrilintide first. Tirzepatide is the primary effective agent.
Most people who think they need this stack actually need plateau troubleshooting. Protein, resistance training, sleep, and hidden calorie audits resolve more stalled weight loss than adding a second drug. Before you add cagrilintide, see why am I not losing weight on tirzepatide and tirzepatide maintenance dose after weight loss. If plateau persists despite optimization, retatrutide (which natively combines GLP-1, GIP, and glucagon) may be a more evidence-backed alternative; see retatrutide vs tirzepatide.
Related Articles: - Cagrilintide Weight Loss Dosage - Tirzepatide Dosage Chart in Units - Retatrutide vs Tirzepatide - Survodutide vs Tirzepatide - Why Am I Not Losing Weight on Tirzepatide - How to Inject Tirzepatide
Related Articles
Cagrilintide Dosage 2026: 22.7% Weight Loss Data
Cagrilintide dosage guide: CagriSema produces 22.7% weight loss at 68 weeks. Titration from 0.25mg to 2.4mg weekly. NDA filed Dec 2025, FDA decision 2026.
CagriSema Dosing Chart (Cagrilintide + Semaglutide)
CagriSema dosing chart and titration. Cagrilintide 0.25-2.4 mg + semaglutide 0.25-2.4 mg, weekly. Not FDA-approved (NDA filed Dec 2025). REDEFINE-1 trial data.
Peptide Dosage Calculator: Units, mL and Vial Math
Peptide dosage calculator hub: work out concentration, volume, and insulin syringe units from any vial, plus the right tool for every peptide dose.
Microdosing GLP-1: What It Is and the Risks
Microdosing GLP-1 means dosing below the range trials tested. What the dose-response data shows, how it differs from titration, and the cost and safety risks.