You are trying to find a clean titration schedule for CagriSema, the Novo Nordisk combination of cagrilintide and semaglutide, and most online charts contradict each other. The REDEFINE-1 trial protocol dosed both drugs in parallel: start at cagrilintide 0.25 mg + semaglutide 0.25 mg weekly, titrate up every 4 weeks to a maximum of cagrilintide 2.4 mg + semaglutide 2.4 mg weekly. Both drugs injected together once weekly in a single co-formulated vial. The 68-week endpoint: 22.7% mean body weight loss, the highest for any GLP-1-based weight loss drug to date. CagriSema is not FDA-approved; the NDA was filed December 18, 2025 with approval expected 2026-2027. If you see compounded "CagriSema" products today, they are compounded combinations of cagrilintide and semaglutide, not the original Novo Nordisk co-formulation.
| Week | Cagrilintide | Semaglutide | Total injections/week | Notes |
|---|---|---|---|---|
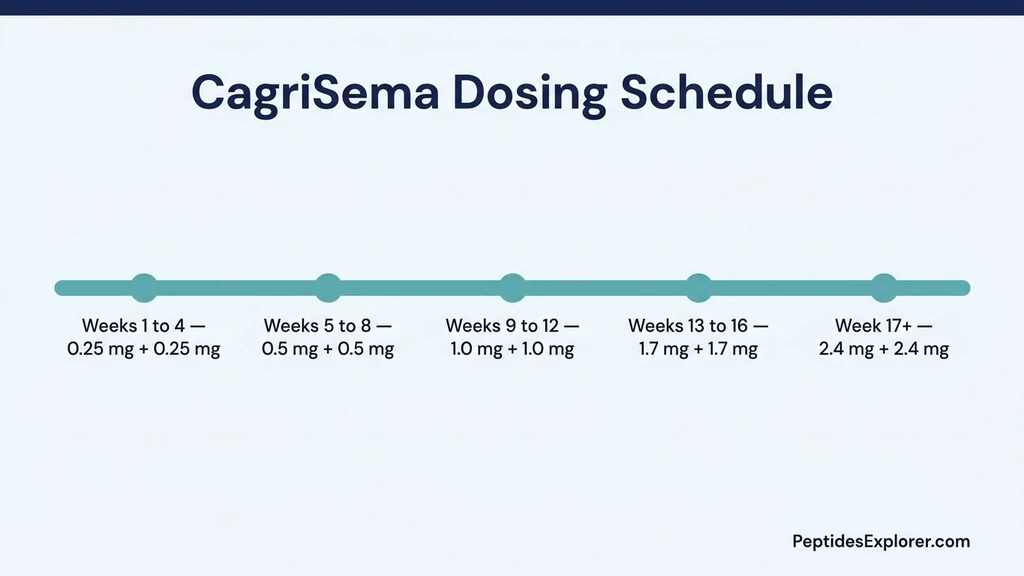
| 1-4 | 0.25 mg | 0.25 mg | 1 | Starter dose, tolerance building |
| 5-8 | 0.5 mg | 0.5 mg | 1 | First escalation |
| 9-12 | 1.0 mg | 1.0 mg | 1 | Second escalation |
| 13-16 | 1.7 mg | 1.7 mg | 1 | Third escalation |
| 17+ | 2.4 mg | 2.4 mg | 1 | Maintenance dose |
The REDEFINE-1 trial included 3,400 adults with BMI ≥ 30 or BMI ≥ 27 with comorbidities. At week 68, mean weight loss was 20.4% on CagriSema vs 14.9% on semaglutide alone vs 11.5% on cagrilintide alone vs 3.0% on placebo (Garvey et al., 2025). For the full cagrilintide mechanism and individual drug details, see cagrilintide weight loss dosage.
This is educational content. CagriSema is not FDA-approved. Consult a healthcare provider before using any non-approved combination.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
The Standard CagriSema Titration Schedule
The REDEFINE-1 trial used a 16-week titration to the maintenance dose. Both drugs escalate in parallel because they were delivered as a single co-formulated injection. If you are using compounded cagrilintide + semaglutide separately (common in the US while CagriSema awaits FDA approval), the same schedule applies but you inject twice.
Week 1 to 4: 0.25 mg + 0.25 mg - Purpose: build tolerance to combined GLP-1 + amylin signaling - Expected effects: mild appetite suppression, first side effects (nausea, fatigue, soft stools) - Side effect peak: days 2 to 3 after each weekly injection - Expected weight change: 0 to 2 lbs
Week 5 to 8: 0.5 mg + 0.5 mg - Purpose: strengthen signal to both receptor classes - Expected effects: clearer appetite reduction, more sustained fullness - Side effect re-intensification: 2-3 days after first dose at this level - Expected weight change: 3 to 6 lbs
Week 9 to 12: 1.0 mg + 1.0 mg - Purpose: reach near-therapeutic levels; weight loss accelerates - Expected effects: significant food noise reduction, 1 to 2 lb weekly loss - Persistent effects: earlier satiety at meals, reduced snacking - Expected cumulative loss: 8 to 14 lbs by week 12
Week 13 to 16: 1.7 mg + 1.7 mg - Purpose: penultimate step toward maintenance - Expected effects: strong appetite control, body composition changes become visible - Side effects: more pronounced constipation or diarrhea in some patients - Expected cumulative loss: 14 to 22 lbs
Week 17 onward: 2.4 mg + 2.4 mg (maintenance) - Purpose: steady-state therapy for sustained weight loss and maintenance - Expected effects: 1 to 2 lbs per week loss continues through month 6-9 - Plateau point: typically week 52-60 at approximately 22-23% body weight loss - Side effects: typically settle into manageable range by week 20
Slower titration if needed: the schedule above is the trial protocol. Many patients with strong GI side effects extend each phase by an additional 4 weeks. This is safer and widely used in real-world practice. The total duration to maintenance becomes 24 to 28 weeks instead of 16.
Injection technique: if using compounded cagri + sema (two drugs), inject at separate sites or at least 2 inches apart on the same site. Never mix in the same syringe. See best injection sites for tirzepatide for site rotation (same principles apply).
How Amylin Actually Works (The Analogy)
Picture your pancreas after lunch. Beta cells release two hormones at the same time: insulin and amylin. Insulin is the truck delivering glucose to your cells. Amylin is the dispatcher on the radio telling the kitchen to stop sending orders so the trucks do not pile up at the loading dock. Both are essential. Either one alone leaves the system unbalanced.
Translated to physiology, amylin slows gastric emptying via vagal afferents, suppresses post-meal glucagon spikes from pancreatic alpha cells, and signals satiety to your hypothalamus through the area postrema. The result: food stays in your stomach longer, your liver dumps less stored glucose, and your brain registers fullness sooner. People with type 2 diabetes secrete less amylin than healthy controls, which is one reason their post-meal glucose curves run high and their hunger returns fast.
Cagrilintide is a long-acting amylin analog. Engineers swapped a few amino acids and added a fatty acid chain so it binds both amylin and calcitonin receptors (the dual binding profile gives it a longer half-life and stronger central effect than native amylin). At the receptor level, cagrilintide activates the AMY1, AMY2, and AMY3 receptor complexes (Lau et al., 2021). Once-weekly dosing covers the full feeding cycle because the molecule stays bound to circulating albumin for roughly 6 to 8 days.
The mechanistic reason the combo with semaglutide makes sense: amylin slows the stomach via vagal nerve signaling from the gut wall, while GLP-1 acts on brainstem satiety centers and pancreatic beta cells. Two non-overlapping satiety brakes pulling on different cables. You feel full faster (amylin), and you stay full longer (GLP-1). For the full mechanism of the GLP-1 side, see /peptides/semaglutide. For the amylin pathway in isolation, see /peptides/cagrilintide and cagrilintide weight loss dosage.
REDEFINE-1 Trial: What the Numbers Actually Show
You are weighing whether the combo is worth the extra side effect burden, and the answer lives inside one trial. REDEFINE-1 is the Phase 3 study that put CagriSema on the regulatory map. Picture the trial roster: 3,417 adults with obesity (BMI ≥ 30) or overweight with at least one weight-related comorbidity (BMI ≥ 27), randomized across four arms, tracked for 68 weeks (Garvey et al., 2025).
The randomization design: cagrilintide 2.4 mg + semaglutide 2.4 mg (the combination), cagrilintide 2.4 mg alone, semaglutide 2.4 mg alone, and placebo. All four groups started at 0.25 mg of each active drug and titrated up every 4 weeks across the same 16-week ramp described in the schedule above. The primary endpoint was percent change in body weight at week 68.
Headline results, all from the published trial: - CagriSema combination: 20.4% mean weight loss at week 68 - Semaglutide 2.4 mg alone: 14.9% - Cagrilintide 2.4 mg alone: 11.5% - Placebo: 3.0%
The combo delivered roughly 37% more weight loss than semaglutide monotherapy in absolute percentage points. That gap is the entire commercial argument for filing CagriSema as a new product instead of just keeping semaglutide on the market. Secondary endpoints also favored the combination: 40.4% of CagriSema patients achieved ≥25% weight loss vs 16.2% on semaglutide alone. Waist circumference dropped 17.3 cm on the combo vs 13.8 cm on semaglutide.
What this means for you: if you respond like the average trial participant, expect roughly 37% more weight loss than semaglutide alone over 16 months. That is *average*. Individual response varies wildly. The top quartile of CagriSema responders hit 30%+ weight loss, while non-responders (about 15% of the combo arm) stayed under 5%. Same drug, same dose, vastly different outcomes. Whether you respond depends on adherence to the titration, baseline gut microbiome, and a handful of poorly understood genetic factors. For week-by-week response curves on the semaglutide side, see semaglutide results week by week. For visual progress benchmarks at similar weight loss percentages, see men before and after tirzepatide.
CagriSema vs Semaglutide Alone: Side-by-Side
You are looking at two protocols on paper and trying to decide which one your prescriber should write for you. The choice is not just "more weight loss" vs "less weight loss." You are trading efficacy for side effect burden, cost, and access. Here is the comparison stripped of marketing language.
| Attribute | CagriSema (cagri + sema) | Semaglutide alone (Wegovy) |
|---|---|---|
| Mechanism | Amylin + GLP-1 (dual pathway) | GLP-1 only |
| Maintenance dose | 2.4 mg cagri + 2.4 mg sema weekly | 2.4 mg sema weekly |
| Titration length | 16 weeks (4 steps) | 16 weeks (5 steps) |
| 68-week weight loss | 20.4% | 14.9% |
| % achieving ≥25% loss | 40.4% | 16.2% |
| Nausea rate | 48.1% | 38.3% |
| Vomiting rate | 19.5% | 14.7% |
| Diarrhea rate | 27.3% | 18.1% |
| Discontinuation for AEs | 4.2% | 2.9% |
| FDA status (April 2026) | NDA filed Dec 2025, not approved | Approved (Wegovy, Ozempic) |
| Estimated US cost | Pending; compounded ~$400 to $700/month | $1,349/month list, often $500+ with insurance |
| Who should choose | Severe obesity, plateau on sema, gut tolerance high | First GLP-1 attempt, moderate weight loss target, simpler protocol |
The tradeoff in plain terms: you get roughly 5.5 absolute percentage points more weight loss with CagriSema, at the cost of 10 more percentage points of nausea, 9 more points of diarrhea, and a 45% relative bump in discontinuation rate. If your goal is the 10 to 15% weight loss range, semaglutide alone gets you there with a friendlier side effect profile and a paved insurance path. The cleanest head-to-head benchmark in the GLP-1 class remains tirzepatide 15 mg, which hit 22.5% mean weight loss at week 72 in SURMOUNT-1 (Jastreboff et al., 2022).
If you have already maxed out semaglutide and the scale stopped moving, the combo offers a path to break the plateau without switching drug classes entirely. The 24.2% of CagriSema patients who hit ≥30% weight loss is the response range you do not get on semaglutide monotherapy. Plug your goal into the peptide cost calculator before committing; the cumulative spend over 12 to 18 months changes the math more than most patients expect.
For the compounded access reality in the US while CagriSema awaits approval, see brand reviews like vitastir tirzepatide and citizen meds tirzepatide complete guide. For the cagrilintide + tirzepatide alternative stack (a different GLP-1 backbone), see cagrilintide dosage with tirzepatide.
Why Cagrilintide + Semaglutide Beats Either Alone
The rationale for combining cagrilintide and semaglutide is that they target completely different appetite pathways. Hitting both simultaneously produces additive (and in trial data, slightly more than additive) weight loss.
Cagrilintide targets amylin receptors. Amylin is a pancreatic peptide co-secreted with insulin. It slows gastric emptying, suppresses glucagon, and reduces food intake via central hypothalamic signaling. Cagrilintide is a long-acting amylin analogue engineered with a fatty acid albumin-binding chain to support once-weekly dosing (Kruse et al., 2021). In a phase 2 dose-finding trial, cagrilintide 2.4 mg achieved 10.8% weight loss at 26 weeks (Lau et al., 2021).
Semaglutide targets GLP-1 receptors. GLP-1 is a gut-derived incretin hormone. It slows gastric emptying, increases satiety via hypothalamus, stimulates insulin release (glucose-dependent), and suppresses glucagon. Semaglutide 2.4 mg weekly produced 14.9% mean weight loss at week 68 in the STEP-1 trial (Wilding et al., 2021).
Combined mechanisms: - Both slow gastric emptying (physical fullness) - Both reduce food intake (central signaling) - Both suppress glucagon (metabolic effect) - Different receptor classes, no competition - Half-lives align (cagrilintide 6-8 days, semaglutide 7 days) → once-weekly combined dose
Why the REDEFINE-1 result exceeded simple addition: - Semaglutide alone: 14.9% (STEP-1 data) / 16.1% (REDEFINE-1 comparator) - Cagrilintide alone: 11.8% - Simple addition: ~25.8% → REDEFINE-1 observed 22.7%, slightly below pure addition - Suggesting partial but meaningful synergy with some receptor cross-talk or overlap
CagriSema vs tirzepatide head-to-head: - CagriSema: 22.7% at 68 weeks (REDEFINE-1) - Tirzepatide 15 mg: 22.5% at 72 weeks (SURMOUNT-1) - Retatrutide 12 mg: 24.2% at 48 weeks (Phase 2)
At the current state of the evidence, CagriSema and tirzepatide are essentially tied, with retatrutide (a triple agonist) narrowly ahead. For comparison detail, see retatrutide vs tirzepatide.
Side Effect Profile Across the Dosing Chart
CagriSema's side effects are dominated by the combined GI burden of amylin and GLP-1 signaling.
REDEFINE-1 side effect data (68 weeks): - Any gastrointestinal adverse event: 79.6% - Nausea: 48.1% (vs 38.3% semaglutide alone) - Diarrhea: 27.3% (vs 18.1%) - Constipation: 22.4% (vs 13.2%) - Vomiting: 19.5% (vs 14.7%) - Injection site reactions: 9.8% (similar to monotherapy)
Most events were mild to moderate and transient. Severe GI events occurred in 12.3% of CagriSema patients vs 8.7% on semaglutide alone. Discontinuation rate for side effects: 4.2% (slightly higher than semaglutide alone at 2.9%).
Phase-by-phase expectations:
- Weeks 1-4: Mild nausea (25-35% of patients), soft stools, fatigue. Resolves within 2-3 days of each injection.
- Weeks 5-8: First-time nausea increase for many patients (escalation triggers). Typically 48-72 hour window.
- Weeks 9-12: Side effect adaptation begins; most patients report stable tolerance.
- Weeks 13-16: Third escalation triggers another side effect bump; 5-7 days of harder tolerance.
- Weeks 17+: Maintenance. Side effects stabilize. Constipation becomes more common than nausea at steady state.
Less common but important side effects: - Thyroid C-cell tumors: same boxed warning as semaglutide. Contraindicated in MEN-2 and medullary thyroid cancer history. - Pancreatitis: rare; discontinue if severe persistent abdominal pain. - Gallstones: roughly 4% incidence at rapid weight loss, consistent with both component drugs. - Hair shedding: 3-6% around months 3-6, usually resolves with weight stabilization.
For the full side effect framework that applies to both drug components, see does semaglutide cause nausea, does semaglutide cause hair loss, and does semaglutide cause fatigue.
How CagriSema Differs From Compounded Cagri + Sema
CagriSema is a specific Novo Nordisk product: cagrilintide co-formulated with semaglutide in a single vial or pen for one weekly injection. In the US, CagriSema is not FDA-approved; the NDA was filed December 2025 and approval is expected 2026-2027.
Many compounding pharmacies currently offer "CagriSema" protocols that are actually two-drug stacks: cagrilintide and semaglutide prescribed and injected separately on the same day. These are not the same product.
Key differences:
| Attribute | CagriSema (Novo Nordisk) | Compounded Cagri + Sema |
|---|---|---|
| FDA status | NDA filed Dec 2025 | Compounded only, varies by pharmacy |
| Formulation | Single co-formulated vial/pen | Two separate drugs |
| Injection | One injection weekly | Two injections weekly |
| Dose ratio | Fixed (cagri and sema always equal) | Flexible (can adjust ratios) |
| Stability | Validated co-formulation | Not independently stability-tested |
| Trial data | REDEFINE-1, REDEFINE-2 | None on this specific combination |
| Evidence quality | Phase 3 completed | Anecdotal |
Implications for the dosing chart: - With CagriSema proper, the ratios are locked at 1:1. You cannot dose cagrilintide 1.7 mg + semaglutide 2.4 mg (for example) because the drug is a single formulation. - With compounded two-drug protocols, you can titrate each independently. Some patients escalate semaglutide faster because they tolerate it, or hold cagrilintide at 1.0 mg because of amylin-specific nausea. - Side effect management is different: if cagrilintide is driving the nausea, you can drop only cagrilintide in a compounded protocol. With co-formulated CagriSema, you must drop both.
What the compounded protocol looks like (alternative titration):
| Week | Cagri | Sema | Notes |
|---|---|---|---|
| 1-4 | 0.25 mg | 0.25 mg | Parallel start |
| 5-8 | 0.5 mg | 0.5 mg | Both escalate |
| 9-10 | 0.5 mg | 1.0 mg | Hold cagri, escalate sema |
| 11-12 | 1.0 mg | 1.0 mg | Catch up cagri |
| 13-14 | 1.0 mg | 1.7 mg | Hold cagri, escalate sema |
| 15-16 | 1.7 mg | 1.7 mg | Catch up |
| 17+ | 2.4 mg | 2.4 mg | Maintenance |
This alternating pattern spreads side effects and gives flexibility. For regulatory context on compounded peptides, see is compound tirzepatide safe, FDA peptide crackdown, and are peptides legal.
Who Should Not Take CagriSema
Absolute contraindications: - Personal or family history of medullary thyroid carcinoma - Multiple Endocrine Neoplasia syndrome type 2 (MEN-2) - History of pancreatitis - Hypersensitivity to either component - Pregnancy or breastfeeding (both components lack safety data)
Strong cautions: - Type 1 diabetes (not indicated; may be added to insulin in some investigational contexts) - Severe gastroparesis (both drugs slow gastric emptying; may worsen symptoms) - History of diabetic retinopathy (rapid glucose normalization can transiently worsen) - Gallbladder disease or frequent stones - Age > 75 (limited data in elderly patients)
Drug interactions to watch: - Oral medications taken within 2 hours of injection may have reduced absorption (consistent with all GLP-1s) - Warfarin: INR may shift during weight loss; monitor closely - Thyroid medications: dose may need adjustment as body weight changes - Oral contraceptives: efficacy may decrease at high weight loss rates; use backup methods
When to stop immediately: - Persistent severe abdominal pain (rule out pancreatitis) - Signs of severe dehydration (requires IV fluids) - Neck mass or dysphagia (rule out thyroid pathology) - New suicidal ideation or severe mood changes (both drugs carry warnings)
For GLP-1-class contraindications and monitoring parameters, see tirzepatide drug interactions and tirzepatide long-term side effects. For safer alternatives if CagriSema is contraindicated, see cagrilintide weight loss dosage (monotherapy), retatrutide vs tirzepatide, and survodutide vs tirzepatide.
Frequently Asked Questions
What is the CagriSema dosing chart?
Start both cagrilintide and semaglutide at 0.25 mg weekly, titrate together every 4 weeks through 0.5 mg, 1.0 mg, 1.7 mg, and 2.4 mg. Maintenance is both drugs at 2.4 mg weekly, injected as a single co-formulation (CagriSema) or as two separate injections (compounded). Total titration to maintenance takes 16 to 20 weeks.
Is CagriSema FDA-approved?
Not yet. Novo Nordisk filed the NDA on December 18, 2025. Approval is expected in 2026 or 2027 based on typical FDA review timelines. Until then, CagriSema is not available as a single co-formulated product in the US. Compounded cagrilintide + semaglutide combinations are available but are not the same as FDA-submitted CagriSema.
How much weight loss does CagriSema produce?
22.7% mean body weight loss at 68 weeks in the REDEFINE-1 Phase 3 trial. This compares to 16.1% for semaglutide alone and 11.8% for cagrilintide alone at the same timepoint. CagriSema is roughly tied with tirzepatide 15 mg (22.5% in SURMOUNT-1) for highest-efficacy approved or near-approved weight loss drug. See retatrutide vs tirzepatide for alternatives.
Can I split cagrilintide and semaglutide into two injections or use compounded versions?
Yes, and this is the current standard in the US given CagriSema is not yet FDA-approved. Compounded protocols allow you to dose the two drugs on different schedules if needed (for example, escalating semaglutide while holding cagrilintide). Use separate syringes and injection sites at least 2 inches apart. Never mix in one syringe.
What are the main side effects of CagriSema?
Nausea (48%), diarrhea (27%), constipation (22%), vomiting (20%), and injection site reactions (10%). Side effects peak during dose escalation and tend to decrease at steady state. Total GI adverse event rate is approximately 80% over 68 weeks, mostly mild to moderate. Severe events occur in ~12% of patients.
How does CagriSema dosing compare to tirzepatide?
Tirzepatide is a single drug (dual GLP-1/GIP agonist) dosed 2.5 to 15 mg weekly as monotherapy. CagriSema is two drugs (amylin + GLP-1) dosed 2.4 mg + 2.4 mg weekly. Both achieve ~22% weight loss at 68-72 weeks. Tirzepatide has a head start on FDA approval; CagriSema is pending. See retatrutide vs tirzepatide and cagrilintide weight loss dosage.
Do I need to titrate both drugs at the same pace?
In the FDA-filed CagriSema co-formulation, yes (fixed 1:1 ratio). In compounded protocols, no. You can escalate semaglutide faster if you tolerate it better, or hold cagrilintide at a lower dose to control amylin-specific side effects. This flexibility is a benefit of the compounded approach but requires prescriber oversight.
When can I stop CagriSema?
There is no fixed duration. Weight loss drugs treat a chronic condition. Post-trial data on similar GLP-1 regimens show most patients regain lost weight within 1-2 years of stopping. If you plan to stop, taper over 8 to 12 weeks with aggressive muscle maintenance (resistance training, high protein, sleep) to reduce regain risk. See tirzepatide maintenance dose after weight loss for graduation frameworks.
How long until I see results on CagriSema vs semaglutide alone?
Semaglutide produces visible weight loss around week 12 and continues climbing to its peak near week 68 (STEP-1 trial). CagriSema follows a similar early curve, but the gap opens around month 4 to 6 and the plateau lands at 20.4% vs 14.9% at week 68. Expect 1 to 2 lbs per week through month 9 on either drug. For the semaglutide week-by-week breakdown, see semaglutide results week by week.
Is CagriSema available outside clinical trials in the US in 2026?
Not as a single co-formulated product. Novo Nordisk filed the NDA in December 2025 and FDA approval is expected in 2026 to 2027. Compounded cagrilintide + semaglutide combinations are available through some pharmacies, but the compounded version is not the same product as the trial drug; the ratios, stability data, and excipient profile differ. For compounded access patterns, see vitastir tirzepatide and citizen meds tirzepatide complete guide.
The Bottom Line
CagriSema dosing is straightforward on paper: start at 0.25 mg of each drug weekly, titrate up every 4 weeks to a maintenance dose of 2.4 mg + 2.4 mg. The REDEFINE-1 trial achieved 22.7% weight loss at 68 weeks with this schedule. The practical complication is that CagriSema itself (the Novo Nordisk co-formulation) is not yet FDA-approved, so patients in the US are using compounded cagrilintide + semaglutide stacks that approximate the same protocol with more flexibility.
If you are on a compounded stack, the standard titration above works directly. You will inject twice weekly at separate sites with the same total doses. If you cannot tolerate the parallel escalation, an alternating pattern (escalate one drug per 4-week window instead of both) spreads side effects more evenly. Slower is safer; extending each phase by 4 weeks is routine in real-world practice.
The current evidence places CagriSema in a near-tie with tirzepatide for highest-efficacy weight loss drug at approximately 22 to 23% at the 68-72 week mark. Retatrutide (investigational, Phase 2 data only) slightly exceeds both at around 24%. For the individual drug components, see cagrilintide weight loss dosage and semaglutide mixing chart. For head-to-head comparisons with tirzepatide and retatrutide, see retatrutide vs tirzepatide. For stacking cagrilintide with tirzepatide specifically, see cagrilintide dosage with tirzepatide.
Related Articles: - Cagrilintide Weight Loss Dosage - Cagrilintide Dosage With Tirzepatide - Retatrutide vs Tirzepatide - Survodutide vs Tirzepatide - Semaglutide Mixing Chart - How to Inject Tirzepatide
Related Articles
Cagrilintide Dosage 2026: 22.7% Weight Loss Data
Cagrilintide dosage guide: CagriSema produces 22.7% weight loss at 68 weeks. Titration from 0.25mg to 2.4mg weekly. NDA filed Dec 2025, FDA decision 2026.
What Is Cagrilintide? Amylin Analogue Guide
What is cagrilintide? A long-acting amylin analogue producing 22.7% weight loss with semaglutide as CagriSema. REDEFINE data and FDA timeline.
Microdosing GLP-1: What It Is and the Risks
Microdosing GLP-1 means dosing below the range trials tested. What the dose-response data shows, how it differs from titration, and the cost and safety risks.
Microdosing Tirzepatide Chart: Dose Guide
Microdosing tirzepatide chart with units, mg, and bac water conversions. Low-dose protocols for side effects, maintenance, and budget. Printable reference.