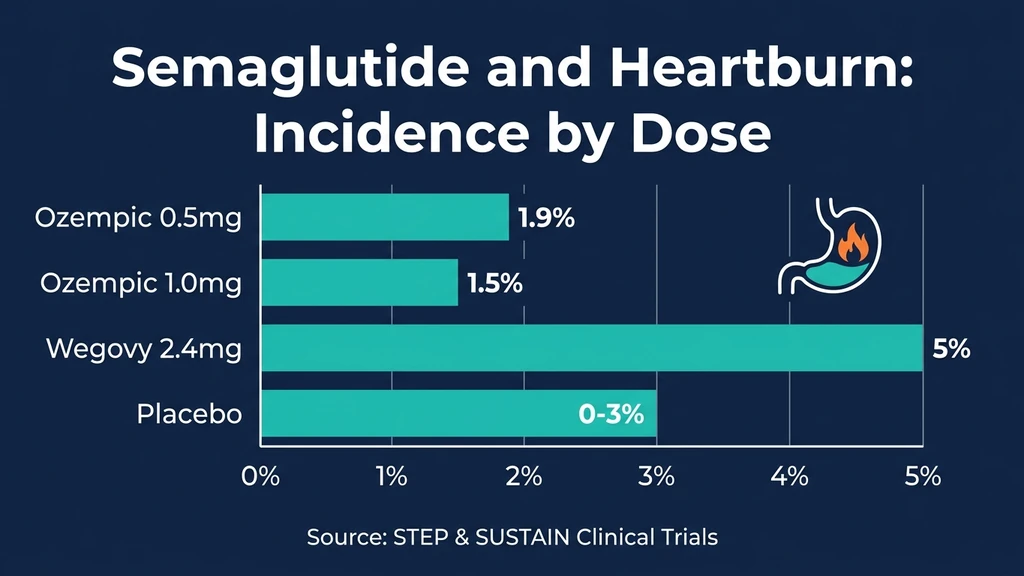
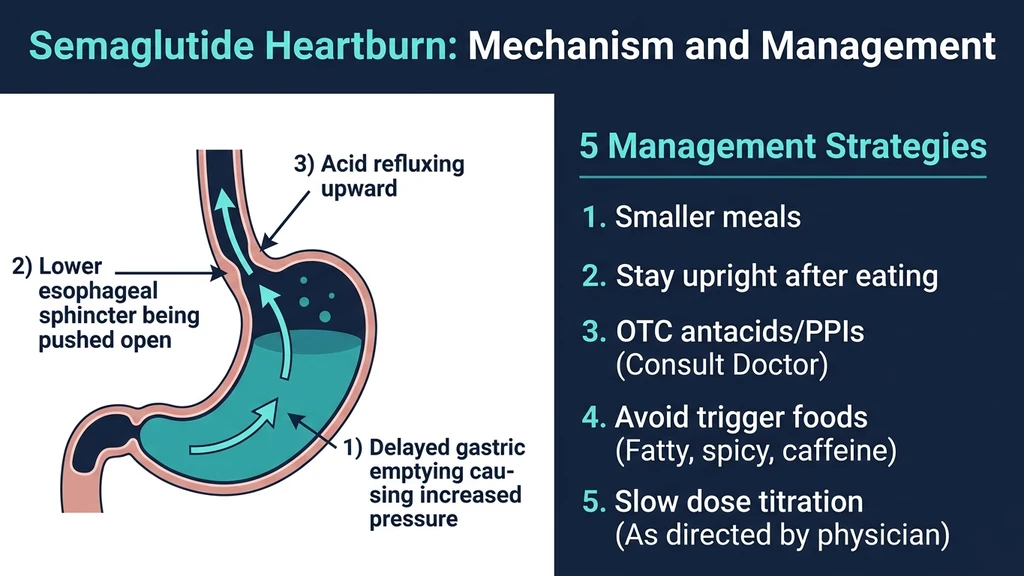
You took your weekly semaglutide injection two days ago. Now a burning sensation rises behind your breastbone every time you eat. Yes, semaglutide can cause heartburn. Clinical trials documented gastroesophageal reflux disease (GERD) in 1.9% of Ozempic users and up to 5% of Wegovy users at the 2.4 mg dose. The drug slows gastric emptying by 30-40%, allowing food and acid to linger in the stomach longer than normal. That extended contact time increases pressure on the lower esophageal sphincter, and when the sphincter yields, acid escapes into the esophagus. The result: heartburn.
For most users, heartburn is temporary. It peaks during dose escalation and fades as the body adjusts over 4-8 weeks. A minority develop persistent GERD requiring medical management. This guide covers the mechanism, clinical incidence data by dose, the distinction between heartburn and GERD, seven management strategies, and when to involve your prescriber.
| Quick Reference | Details |
|---|---|
| Prevalence | 1.9% (Ozempic 0.5 mg), 1.5% (Ozempic 1.0 mg), 5% (Wegovy 2.4 mg) vs 0-3% placebo |
| Cause | Delayed gastric emptying increases intragastric pressure on the lower esophageal sphincter |
| Onset | 1-7 days after first dose or dose increase |
| Peak severity | First 2-4 weeks at each new dose level |
| Resolution | 4-8 weeks at a stable dose for most users |
| Key fix | Smaller meals, upright posture, OTC antacids or PPIs, slow titration |
| Evidence level | Human clinical trials (STEP 1-5, SUSTAIN 1-10) + population cohort studies |
For dosing protocols, see our semaglutide dosage chart. For safety information, see our peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Semaglutide Causes Heartburn: The Mechanism
Think of your stomach as a pressure cooker with a one-way valve at the top. That valve is the lower esophageal sphincter (LES), a ring of smooth muscle that opens to let food in and closes to keep acid out. Under normal conditions, your stomach empties its contents into the small intestine within 2-4 hours, and the pressure inside stays low enough that the LES holds firm. Semaglutide changes both variables.
The drug activates GLP-1 receptors on vagal nerve endings in the stomach wall. Those receptors send a signal that relaxes the pyloric sphincter less frequently and reduces the contractions that push food forward. Gastric emptying slows by 30-40%. A meal that used to clear in 3 hours now sits for 4-5. The longer food remains, the more gastric acid the parietal cells secrete, and the greater the volume and pressure inside the stomach (Nauck et al., 2021).
When intragastric pressure rises high enough, it overwhelms the LES. Acid and partially digested food reflux upward into the esophagus, which lacks the stomach's protective mucus lining. The esophageal nerve endings register the acid as a burning sensation. That is heartburn.
Three factors make semaglutide users more vulnerable than the general population:
1. Prolonged acid contact time. A slow-emptying stomach keeps hydrochloric acid in contact with the gastric mucosa and the LES for hours longer than normal. The LES fatigues under sustained pressure.
2. Increased meal-related distension. Users who eat their usual portions on semaglutide overfill a stomach that has not cleared the previous meal. The mechanical stretch adds to the pressure differential across the LES.
3. Nausea-induced vomiting. Semaglutide causes nausea in 44% of users at the 2.4 mg dose. Repeated vomiting forces acid past the LES repeatedly. A 2025 case report documented severe reflux esophagitis caused by GLP-1 agonist-induced vomiting, with endoscopy revealing Los Angeles grade C esophagitis that required hospitalization (Noguchi et al., PMC 2025).
Semaglutide does not directly weaken the LES. The sphincter muscle itself functions normally. The problem is purely mechanical: too much pressure for too long on the stomach side of the valve.
Heartburn Incidence by Dose: Clinical Trial Data
The STEP and SUSTAIN clinical trial programs provide the clearest data on heartburn and GERD rates across semaglutide doses. The pattern is consistent: higher doses produce more reflux, but absolute rates remain low compared to other GI side effects like nausea and diarrhea.
Ozempic (Diabetes Indication, 0.5-1.0 mg):
The SUSTAIN trials enrolled over 8,000 patients with type 2 diabetes. GERD was reported in 1.9% of patients at 0.5 mg and 1.5% at 1.0 mg, compared to 0% on placebo in some trials. This makes heartburn a relatively uncommon side effect at diabetes-indication doses (Novo Nordisk, Ozempic prescribing information).
Wegovy (Obesity Indication, 2.4 mg):
The STEP 1 trial documented GERD in approximately 5% of users at the 2.4 mg dose versus 3% on placebo. The absolute risk increase is 2 percentage points. Most cases were classified as mild to moderate. Fewer than 0.5% of participants discontinued treatment because of reflux symptoms (Wilding et al., NEJM 2021).
Real-World Data (Shu et al.):
A pharmacovigilance analysis of semaglutide-related adverse events found serious GERD at 2.64% and non-serious GERD at 3.28%. These rates are higher than clinical trial estimates, likely because real-world patients include those with pre-existing reflux, hiatal hernias, and other risk factors excluded from controlled trials.
Population Cohort Study (2025):
The largest observational study to date compared 24,708 GLP-1 receptor agonist users to 89,096 SGLT-2 inhibitor users with type 2 diabetes. Over a median 3.0-year follow-up, GLP-1 users had a hazard ratio of 1.27 (95% CI: 1.14-1.42) for new GERD diagnosis. The risk difference was 0.7 per 100 patients. The risk of GERD complications (stricture, Barrett's esophagus) was even higher: HR 1.55 (95% CI: 1.12-2.29). Risk was elevated for all GLP-1 agonists except lixisenatide (Annals of Internal Medicine, 2025).
| Formulation | Dose | GERD Rate | Placebo/Comparator | Risk Increase |
|---|---|---|---|---|
| Ozempic | 0.5 mg | 1.9% | 0% | +1.9 pp |
| Ozempic | 1.0 mg | 1.5% | 0% | +1.5 pp |
| Wegovy | 2.4 mg | 5.0% | 3.0% | +2.0 pp |
| Real-world | Mixed | 3.3-5.9% | N/A | Variable |
| Cohort (3 yr) | Mixed | HR 1.27 | SGLT-2 users | +0.7 per 100 |
For context, nausea affects 44% and diarrhea affects 30% at the 2.4 mg dose. Heartburn at 5% is among the less common GI side effects, but its chronic nature and potential for esophageal damage make it worth monitoring closely.
Heartburn vs. GERD: Understanding the Difference
The terms are used interchangeably in casual conversation, but clinically they describe different conditions. The distinction matters because GERD requires a different management approach and carries risks that occasional heartburn does not.
Occasional Heartburn
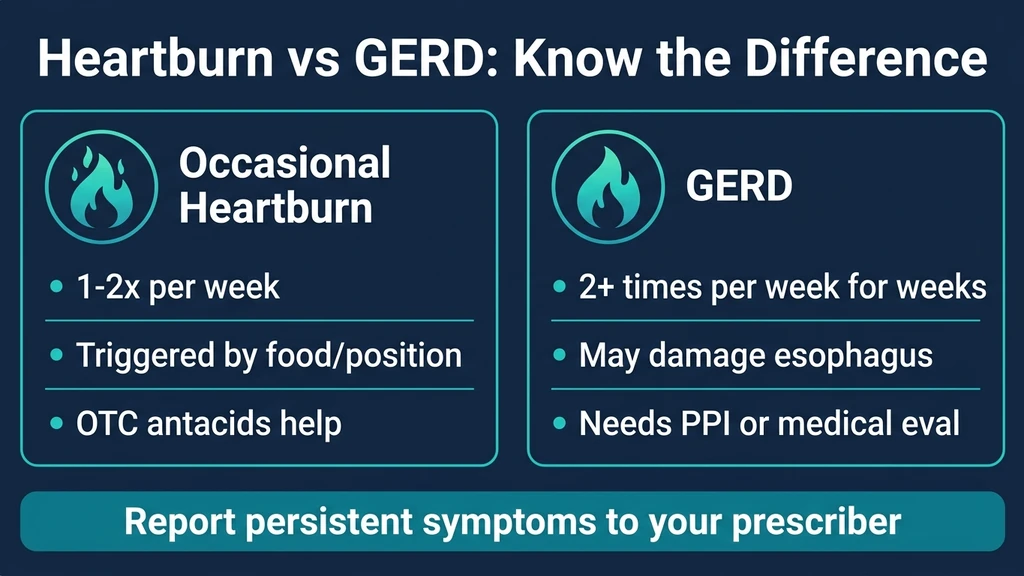
Heartburn is a symptom: a burning sensation behind the breastbone that rises toward the throat. It occurs when stomach acid contacts the esophageal lining. Nearly everyone experiences it at some point. On semaglutide, occasional heartburn typically happens after large meals, when lying down too soon after eating, or during the first 2-4 weeks at a new dose.
Key features of occasional heartburn on semaglutide: - Occurs fewer than 2 times per week - Triggered by specific foods (spicy, fatty, acidic) or body position - Resolves with over-the-counter antacids (Tums, Gaviscon) within 30 minutes - Does not wake you from sleep regularly - Improves as your body adjusts to the current dose
Occasional heartburn does not damage the esophagus. It is uncomfortable but benign. Most semaglutide users who report heartburn fall into this category.
Gastroesophageal Reflux Disease (GERD)
GERD is a chronic condition defined by acid reflux occurring 2 or more times per week for several weeks. The repeated acid exposure damages the esophageal lining, potentially causing erosive esophagitis, strictures, or Barrett's esophagus (a precancerous cell change).
Symptoms that distinguish GERD from occasional heartburn: - Burning occurs 2+ times per week for 4+ weeks - Acid regurgitation: sour or bitter fluid reaching the throat or mouth - Difficulty swallowing (dysphagia) or pain when swallowing - Chronic cough, hoarseness, or sore throat without infection - Chest pain that worsens when lying flat - Nighttime symptoms that disrupt sleep - Symptoms persist despite antacid use
If semaglutide triggers any of these patterns, stop treating it as routine heartburn. The 2025 population cohort study found that GLP-1 users had a 55% higher risk of GERD complications compared to SGLT-2 inhibitor users. Risk was particularly elevated among smokers, patients with obesity, and those with pre-existing gastric conditions (Annals of Internal Medicine, 2025).
Contact your prescriber if symptoms meet the GERD criteria. Standard treatment is a proton pump inhibitor (PPI) such as omeprazole 20 mg once daily. In most cases, semaglutide can be continued alongside a PPI without dose adjustment.
Risk Factors That Increase Heartburn on Semaglutide
Not everyone on semaglutide develops heartburn. Certain factors make it more likely:
Pre-existing GERD or hiatal hernia. A weakened LES or anatomical displacement of the stomach above the diaphragm compounds the pressure that delayed gastric emptying creates.
Obesity. Excess abdominal fat increases baseline intra-abdominal pressure. Semaglutide is commonly prescribed for obesity, so this risk factor applies to a large portion of users. The paradox: semaglutide treats the condition (obesity) that worsens one of its side effects (heartburn). As weight loss progresses, heartburn often improves.
Smoking. Nicotine relaxes the LES. Smokers on semaglutide face the combined effect of a relaxed valve and increased gastric pressure.
Concurrent medications. NSAIDs (ibuprofen, naproxen), calcium channel blockers, certain antidepressants, and bisphosphonates all worsen reflux. Review your full medication list with your prescriber.
Large meal sizes. This is the most modifiable risk factor. A stomach slowed by semaglutide that receives a 1,000-calorie meal will generate far more pressure than one receiving 400 calories.
When Does Semaglutide Heartburn Start and Stop?
Heartburn follows a timeline linked to dose changes and gastric adaptation. Understanding this pattern helps you distinguish normal adjustment from a worsening condition.
Onset: Days 1-7 After a Dose Change
Heartburn most commonly appears within the first week of starting semaglutide or increasing the dose. The drug reaches peak plasma concentration 1-3 days after injection. As levels rise, gastric emptying slows progressively. Users who ate their usual portions during this window often experienced the first reflux episode after a large dinner followed by lying on the couch.
The 0.25 mg starting dose rarely causes heartburn. The 0.5 mg to 1.0 mg transition is the most common trigger because it doubles the degree of gastric slowing. For timing context on other side effects at this transition, see how long do semaglutide side effects last.
Peak: Weeks 1-4 at Each New Dose
Heartburn intensity peaks during the first month at each dose level. Semaglutide has a half-life of approximately 7 days, reaching steady-state plasma levels after 4-5 weeks. During this accumulation phase, gastric emptying slows progressively. Weeks 2-3 at a new dose are typically the worst for reflux.
Users report 2-5 heartburn episodes per week during this window, often after dinner or when lying down. The episodes respond to antacids but recur the next day.
Improvement: Weeks 4-8
The gastrointestinal tract partially adapts to sustained GLP-1 stimulation. Gastric emptying remains slower than baseline but the degree of slowing attenuates. The STEP 5 two-year extension data showed that most GI adverse events, including reflux, were concentrated in the first 20 weeks of treatment and declined steadily thereafter (Garvey et al., Nature Medicine 2022).
By 4-8 weeks at a stable dose, the majority of users with mild heartburn report resolution or significant improvement. If heartburn persists unchanged beyond 8 weeks at the same dose, it may indicate true GERD requiring treatment rather than transient drug adaptation.
Long-Term: Weight Loss May Help
An underappreciated benefit: as semaglutide produces weight loss over months, intra-abdominal pressure decreases. For patients whose heartburn stemmed partly from obesity, losing 10-15% of body weight can reduce reflux episodes by 40-60%. Some users find that heartburn was worst at the beginning of treatment and disappeared entirely after 20-30 pounds of weight loss, even at higher doses. If you are tracking your weight loss progress, our semaglutide dosage calculator can help ensure your dose is optimized.
7 Strategies to Manage Heartburn on Semaglutide
These strategies are ordered from most impactful to supplementary. The first three alone resolve heartburn in the majority of cases.
1. Eat Smaller, More Frequent Meals
This is the single most effective change. A stomach slowed by semaglutide cannot handle the same volume it did before treatment. Switch from 2-3 large meals to 4-5 smaller ones spaced 3-4 hours apart. Keep each meal under 400-500 calories. Smaller volume means less gastric distension, less pressure on the LES, and less acid production.
A practical test: if your heartburn follows dinner (the largest meal for most people), split dinner into two smaller meals eaten 3 hours apart. Many users find this single adjustment eliminates evening heartburn entirely. For nutritional guidance during treatment, see not losing weight on semaglutide for dietary strategies that also reduce GI side effects.
2. Stay Upright for 2-3 Hours After Eating
Gravity is a free anti-reflux mechanism. When you stand or sit upright, gastric contents pool at the bottom of the stomach, away from the LES. When you lie down, the acid level rises to the LES level and reflux becomes almost inevitable in a slow-emptying stomach.
Do not eat within 3 hours of bedtime. If you eat dinner at 7 PM, do not lie down before 10 PM. Elevate the head of your bed 6-8 inches using bed risers or a foam wedge pillow. Regular pillows are insufficient because they bend the neck without elevating the entire torso. The 6-8 inch incline keeps the LES above the gastric acid pool throughout the night.
3. Avoid Known Reflux Triggers
Certain foods relax the LES or increase acid production. On semaglutide, their effect is amplified because the stomach is already under pressure:
Foods to limit or avoid during dose escalation: - Fatty and fried foods (slow digestion further) - Spicy foods (capsaicin irritates the esophageal lining) - Citrus fruits and tomato-based sauces (acidic) - Chocolate (contains methylxanthine, which relaxes the LES) - Coffee and caffeinated beverages (stimulate acid secretion) - Carbonated drinks (increase gastric volume and pressure) - Alcohol (relaxes the LES and increases acid production) - Peppermint (relaxes smooth muscle including the LES)
Favor lean proteins (chicken breast, white fish), complex carbohydrates (rice, oatmeal, whole grain bread), and cooked vegetables. Bananas, melons, and ginger are traditionally well-tolerated by reflux patients.
4. Use Over-the-Counter Antacids for Acute Episodes
For occasional heartburn, OTC antacids provide rapid relief:
Calcium carbonate (Tums, Rolaids): Neutralizes stomach acid within 5 minutes. Duration: 30-60 minutes. Best for infrequent, mild episodes. Take as needed, up to 4-6 tablets daily.
Alginate-based (Gaviscon): Forms a physical raft on top of the stomach contents that blocks acid from reaching the LES. Lasts 2-4 hours. Particularly effective when taken after meals and before bed.
H2 receptor blockers (famotidine/Pepcid): Reduces acid production for 8-12 hours. Take 20 mg before dinner or at bedtime. Works as preventive rather than rescue therapy.
If you need antacids more than 2-3 times per week, move to strategy 5.
5. Proton Pump Inhibitors (PPIs) for Persistent Reflux
PPIs are the standard treatment when heartburn becomes frequent. They block the proton pump in parietal cells, reducing stomach acid production by 90%. No known interactions with semaglutide.
Standard regimen: Omeprazole 20 mg (or equivalent PPI) once daily, taken 30 minutes before breakfast. If inadequate after 2 weeks, escalate to twice daily (before breakfast and before dinner). Most guidelines recommend using the lowest effective dose for the shortest necessary duration.
A clinical management review recommends starting PPI therapy at once-daily dosing for GERD in semaglutide users, escalating to twice-daily only if needed (DrOracle Clinical Review, 2025).
PPIs are safe for long-term use but carry small risks with chronic use: reduced calcium and magnesium absorption, slightly increased pneumonia risk, and possible vitamin B12 deficiency. Discuss duration with your prescriber.
6. Follow the Titration Schedule Strictly
Dose escalation is the primary driver of new heartburn episodes. Each increase in semaglutide concentration deepens the gastric emptying delay. The standard titration (0.25 mg for 4 weeks, then 0.5 mg, then 1.0 mg, then 1.7 mg, then 2.4 mg) gives the stomach 4 weeks to adapt at each level.
Skipping a dose level or increasing faster than every 4 weeks compresses the adaptation window. The STEP 2 trial showed lower GI side effect rates at sites that used slower titration protocols. If heartburn is problematic, stay at the current dose for an extra 2-4 weeks before escalating. Some users find that microdosing semaglutide with intermediate dose steps reduces reflux during transitions.
Weight loss still occurs at lower doses. There is no penalty for titrating slowly. A patient who stays at 1.0 mg for 8 weeks instead of 4 will still reach their target dose, with less heartburn along the way.
7. Lose Weight (the Long-Term Solution)
This sounds circular (you are taking semaglutide to lose weight), but the timeline matters. Heartburn is worst in the first weeks and months of treatment when the drug's gastric effects are strongest and body weight is still high. As weight drops, intra-abdominal pressure decreases, the mechanical load on the LES lightens, and reflux episodes decline.
A meta-analysis of bariatric outcomes found that every 5% reduction in body weight reduced GERD symptom scores by 15-20%. Patients who lost 15%+ of body weight (a common outcome on semaglutide 2.4 mg) frequently experienced complete resolution of pre-existing GERD. The drug that initially worsened reflux ultimately treats the root cause.
For patients struggling with weight loss on the drug, see not losing weight on semaglutide for plateau-breaking strategies.
Semaglutide and Pre-Existing GERD: Can You Still Take It?
Yes, in most cases. Pre-existing GERD is not a contraindication to semaglutide. However, it requires proactive management.
Before starting semaglutide with existing GERD: - Ensure your GERD is controlled on current therapy (PPI, lifestyle modifications) - Inform your prescriber about the severity and frequency of your reflux - Consider starting at the lowest dose (0.25 mg) with a slower titration - Have a rescue plan: keep Gaviscon or famotidine available for breakthrough symptoms
During treatment: - Monitor symptoms at each dose increase. A temporary worsening (2-4 weeks) is expected - Do not stop your PPI when starting semaglutide - If symptoms worsen significantly, delay dose escalation rather than stopping semaglutide - Weight loss from semaglutide often improves underlying GERD over 3-6 months
When to reconsider semaglutide: - Symptoms escalate to Los Angeles grade C/D esophagitis despite maximal PPI therapy - New-onset dysphagia (difficulty swallowing) that worsens despite treatment - Recurrent vomiting causing dehydration (this overlaps with semaglutide's nausea effect; for management see how to relieve nausea from semaglutide) - Endoscopic finding of Barrett's esophagus progression
For most patients with mild-to-moderate GERD, the long-term weight loss benefit outweighs the short-term reflux worsening. A structured discussion with your gastroenterologist and prescriber can weigh the risks. For broader guidance on medication safety, see our peptide safety guide.
Semaglutide vs. Tirzepatide: Which Causes More Heartburn?
Tirzepatide (Mounjaro, Zepbound) is a dual GIP/GLP-1 receptor agonist that shares the gastric-slowing mechanism with semaglutide. Both drugs delay gastric emptying and both can cause heartburn. Head-to-head data comparing reflux rates are limited, but the available evidence suggests similar or slightly lower rates with tirzepatide.
The SURMOUNT trials reported GERD in approximately 3-4% of tirzepatide users at the highest dose (15 mg) compared to 5% for semaglutide 2.4 mg in STEP 1. The GIP receptor component of tirzepatide may partially offset the GLP-1-mediated gastric slowing, though this mechanism remains under investigation.
Users switching between the two drugs should expect a possible flare of heartburn during the transition period as the body adjusts to a different receptor activation pattern. For equivalent dosing when switching, see our semaglutide to tirzepatide conversion guide.
Neither drug is clearly better or worse for heartburn. The choice between semaglutide and tirzepatide should be based on overall efficacy, tolerability, cost, and insurance coverage rather than heartburn risk alone.
What Does the Research Say?
The evidence base for semaglutide and heartburn spans controlled clinical trials, pharmacovigilance databases, and population-level cohort studies.
Clinical Trial Evidence
STEP 1 (Wilding et al., 2021): 1,961 adults with obesity. GERD reported in approximately 5% of semaglutide 2.4 mg users vs 3% placebo. Most cases mild (grade 1-2). Discontinuation due to reflux: less than 0.5% (PubMed).
SUSTAIN Trials (2017-2020): Over 8,000 patients with type 2 diabetes. GERD in 1.5-1.9% at 0.5-1.0 mg doses. The lower incidence reflects the lower doses used for diabetes versus obesity (PubMed).
STEP 5 (Garvey et al., 2022): Two-year extension data showed that GI adverse events including reflux were most frequent during the first 20 weeks and declined significantly by year two. This confirms gastric adaptation over time (Nature Medicine).
Mechanistic Studies
Gastric Emptying (Halawi et al., 2023): Semaglutide delays 4-hour gastric emptying in women with obesity, confirming the mechanism linking the drug to increased gastric pressure and reflux risk (PubMed).
GLP-1 Receptor Review (Nauck et al., 2021): Comprehensive review confirming GLP-1 agonists slow gastric emptying by 30-40% via vagal nerve pathways. Effect partially attenuates over 4-8 weeks. The attenuation is incomplete, which is why some users retain reflux symptoms long-term while appetite suppression persists (PubMed).
FAERS Pharmacovigilance (Wang et al., 2022): Analysis of the FDA Adverse Event Reporting System found GERD-like symptoms disproportionately reported with semaglutide (reported odds ratio 5.61) compared to non-GLP-1 medications (PMC).
Population-Level Evidence
GLP-1 RA vs SGLT-2 Cohort (Annals of Internal Medicine, 2025): 24,708 GLP-1 RA users vs 89,096 SGLT-2 inhibitor users. Median follow-up 3.0 years. Risk ratio for GERD: 1.27 (95% CI: 1.14-1.42). Risk ratio for GERD complications: 1.55 (95% CI: 1.12-2.29). Risk elevated for all GLP-1 agents except lixisenatide. Notably higher among smokers, patients with obesity, and those with gastric comorbidities (PubMed).
Shorter-Acting GLP-1 RA Study (Abrahami et al., 2023): Population-level matched cohort finding that shorter-acting GLP-1 receptor agonists were associated with higher GERD development and complications compared to longer-acting formulations. Semaglutide, as a long-acting weekly injection, may carry somewhat lower reflux risk than older twice-daily GLP-1 agents (PubMed).
Systematic Review and Meta-Analysis (Gastroenterology, 2025): Pooled analysis of GLP-1 RA trials confirmed a statistically significant increase in GI adverse events including GERD. The meta-analysis estimated that for every 100 patients treated with a GLP-1 RA, approximately 1 additional patient develops GERD compared to alternative glucose-lowering therapies (Gastroenterology).
Important Warnings
Severe esophagitis from vomiting. Semaglutide-induced vomiting can cause acute reflux esophagitis severe enough to require hospitalization. A 2025 case report documented Los Angeles grade C esophagitis in a patient on a GLP-1 agonist who experienced repeated vomiting. Endoscopy revealed significant mucosal damage (PMC 2025). If you are vomiting more than 2-3 times per day, contact your prescriber. For strategies to control vomiting, see how to relieve nausea from semaglutide.
Do not ignore dysphagia. Difficulty swallowing (food "sticking" in the throat or chest) on semaglutide may indicate esophageal narrowing from chronic acid damage. This is rare but requires prompt endoscopic evaluation.
Alarm symptoms requiring immediate evaluation: - Vomiting blood or black/tarry stools (upper GI bleeding) - Unintentional weight loss beyond what semaglutide explains - Severe chest pain (must differentiate cardiac vs esophageal) - Persistent hoarseness or chronic cough without respiratory cause - Heartburn that worsens steadily despite PPI therapy
Drug interactions with antacids. While PPIs and H2 blockers are safe with semaglutide, aluminum-containing antacids can theoretically slow absorption of some oral medications. Since semaglutide is injected, this is not a direct concern for the drug itself, but review your full medication list for oral drugs whose absorption may be affected.
Because semaglutide stays in your system for approximately five weeks after your last injection, heartburn may persist for several weeks after discontinuation. Do not expect immediate relief upon stopping the drug.
Related Side Effects
Heartburn rarely occurs in isolation on semaglutide. It shares a mechanistic root (altered GI motility) with several other side effects. Understanding the overlap helps you and your prescriber address the full picture.
Does Semaglutide Cause Nausea? Nausea (44% incidence at 2.4 mg) and heartburn share the same trigger: delayed gastric emptying. Managing one often improves the other. Smaller meals and upright posture reduce both.
Can Semaglutide Cause Diarrhea? Diarrhea (30% at 2.4 mg) operates through a different colonic mechanism but often occurs alongside heartburn during dose escalation. The combination of upper GI (heartburn) and lower GI (diarrhea) symptoms is common during the first month.
Does Semaglutide Cause Fatigue? Fatigue (11% incidence) can worsen when heartburn disrupts sleep. Nighttime reflux interrupts sleep architecture, contributing to daytime exhaustion. Elevating the head of the bed addresses both issues.
How Long Do Semaglutide Side Effects Last? Comprehensive timeline covering all major side effects, including how heartburn fits into the broader adaptation curve during titration.
Peptides for Gut Health For users interested in supporting GI health during GLP-1 therapy, this guide covers peptides with gut-protective properties including BPC-157 and others that may complement digestive function.
Frequently Asked Questions
How common is heartburn on Ozempic vs Wegovy?
Ozempic (0.5-1.0 mg for diabetes) causes GERD in 1.5-1.9% of users. Wegovy (2.4 mg for weight loss) causes it in approximately 5%. The difference is dose-dependent: Ozempic and Wegovy contain the same molecule (semaglutide), but Wegovy uses a higher dose that produces greater gastric emptying delay and more pressure on the lower esophageal sphincter.
Can I take Tums or Gaviscon while on semaglutide?
Yes. Over-the-counter antacids including calcium carbonate (Tums), alginate-based formulas (Gaviscon), and H2 blockers (famotidine/Pepcid) are safe to use with semaglutide. Because semaglutide is injected, antacids do not affect its absorption. Gaviscon is particularly effective because it creates a physical barrier that prevents acid from reaching the esophagus. For a broader view of drug compatibility, see our peptide safety guide.
Will semaglutide heartburn go away on its own?
For most users, yes. Heartburn peaks during the first 2-4 weeks at each new dose and improves as the GI tract adapts over 4-8 weeks. STEP 5 two-year data confirmed that GI adverse events decline significantly after the initial 20-week titration period. If heartburn persists unchanged beyond 8 weeks at a stable dose, consult your prescriber, as this may indicate GERD requiring proton pump inhibitor therapy.
Should I stop semaglutide because of heartburn?
Rarely. Heartburn alone is almost never a reason to discontinue semaglutide. It responds well to lifestyle modifications, antacids, or PPIs in the vast majority of cases. Discontinuation should only be considered if you develop severe complications like refractory esophagitis, Barrett's esophagus progression, or esophageal stricture despite maximal anti-reflux therapy. Your prescriber can adjust the semaglutide dosage or slow the titration schedule instead of stopping.
Does semaglutide make existing GERD worse?
It can temporarily worsen GERD symptoms, especially during dose escalation. The 2025 population cohort study found a 27% increased risk of new GERD diagnosis in GLP-1 users. However, patients with well-controlled GERD on PPI therapy can usually continue semaglutide safely. Maintain your current GERD medications, avoid trigger foods, and use a slower titration schedule. Long-term weight loss from semaglutide often improves underlying GERD by reducing intra-abdominal pressure.
Is heartburn from semaglutide dangerous?
Occasional heartburn is uncomfortable but not dangerous. Chronic, unmanaged GERD carries risks including esophageal erosion, strictures, and Barrett's esophagus (a precancerous condition). The 2025 cohort study found a 55% increased risk of GERD complications in GLP-1 users over 3 years. The key is monitoring: treat persistent heartburn (2+ times per week for 4+ weeks) with PPIs and inform your prescriber. For comprehensive safety information, see our peptide safety guide.
What is the best sleeping position for semaglutide heartburn?
Elevate the head of your bed 6-8 inches using bed risers or a foam wedge pillow. Sleep on your left side. This combination keeps the gastroesophageal junction above the acid pool and positions the stomach below the esophagus. Regular pillows are not effective because they bend the neck without elevating the torso. Do not eat within 3 hours of bedtime. These measures, combined with smaller evening meals, resolve nighttime heartburn for most semaglutide users.
Does tirzepatide cause less heartburn than semaglutide?
Possibly, but the data are limited. The SURMOUNT trials reported GERD in approximately 3-4% of tirzepatide users at 15 mg versus 5% for semaglutide 2.4 mg in STEP 1. Tirzepatide's dual GIP/GLP-1 mechanism may partially offset GLP-1-mediated gastric slowing. However, no head-to-head trial has specifically compared reflux rates. The choice between drugs should weigh overall efficacy, tolerability, and cost rather than heartburn risk alone.
The Bottom Line
Semaglutide causes heartburn in 1.9-5% of users depending on dose. The mechanism is straightforward: delayed gastric emptying increases stomach volume and pressure, overwhelming the lower esophageal sphincter and allowing acid into the esophagus. Most cases are mild, peak during dose escalation, and resolve within 4-8 weeks at a stable dose.
Seven strategies reduce heartburn: smaller meals, upright posture after eating, avoiding trigger foods, OTC antacids for acute episodes, PPIs for persistent reflux, strict adherence to the titration schedule, and long-term weight loss. For most users, the first three are sufficient.
Pre-existing GERD is not a contraindication. Continue your PPI, inform your prescriber, and titrate slowly. The long-term weight loss that semaglutide delivers often improves underlying GERD by reducing intra-abdominal pressure.
Monitor for GERD warning signs: symptoms more than twice weekly, acid regurgitation, dysphagia, or nighttime awakening from reflux. These require medical evaluation and treatment. Heartburn alone is almost never a reason to discontinue semaglutide.
Use our semaglutide dosage calculator to plan your titration schedule. For dosing details, see our semaglutide dosage chart in mL. For the full side effect timeline, read how long do semaglutide side effects last.
Related Articles: - Does Semaglutide Cause Nausea? - 44% incidence, shared mechanism with heartburn - Can Semaglutide Cause Diarrhea? - 30% incidence, colonic GLP-1 activation - Does Semaglutide Cause Fatigue? - nighttime reflux disrupts sleep - How to Relieve Nausea from Semaglutide - overlapping management strategies - Peptides for Gut Health - GI support during GLP-1 therapy - Semaglutide Dosage Chart - titration schedule reference - Peptide Safety Guide - comprehensive safety overview
Related Articles
Can Semaglutide Cause Diarrhea?
Diarrhea affects 8-30% of semaglutide users depending on dose. Learn the GLP-1 mechanism, STEP trial incidence data, timeline, and 6 management strategies.
Does Semaglutide Cause Nausea?
Nausea affects 40-45% of semaglutide users, especially during dose titration. Learn the mechanism, timeline, and 5 proven strategies to reduce it.
Can Semaglutide Cause Depression?
Clinical trials show semaglutide does not increase depression risk. FDA cleared GLP-1 drugs of suicidality concerns in 2025. Evidence and mechanisms.
Semaglutide Nausea Relief: 9 Proven Tips
Relieve semaglutide nausea with 9 actionable strategies: ondansetron dosing, ginger protocols, dietary timing, acupressure, and when to call your doctor.