You stepped on the scale and celebrated losing 50 pounds on Mounjaro. Then your trainer measured your grip strength and it dropped 20%. You are wondering if the drug is eating your muscle along with the fat. Yes, tirzepatide causes lean mass loss. SURMOUNT-1 DEXA data showed that 25% of total weight lost was lean mass and 75% was fat mass, translating to 5.6 kg of lean tissue lost over 72 weeks (Look et al., Diabetes Obes Metab, 2025). That ratio is better than semaglutide (39% lean mass loss) and consistent with any caloric deficit without resistance training.
| Quick Reference | Details |
|---|---|
| Does tirzepatide cause muscle loss? | Yes. 25% of weight lost is lean mass |
| Absolute lean mass lost | 5.6 kg (12.3 lb) at 72 weeks |
| Fat mass lost | 15.9 kg (35 lb) at 72 weeks |
| Fat-to-lean loss ratio | 3:1 (75% fat, 25% lean) |
| Worse than semaglutide? | No. Semaglutide loses 39% lean mass vs 25% |
| Primary prevention | Protein 1.2 to 1.6 g/kg + resistance training 2 to 3x/week |
| Supplement evidence | Creatine: strong. HMB: moderate. Leucine: supportive |
| Evidence level | SURMOUNT-1 DEXA substudy (n=160), SURPASS-3 MRI substudy |
For dosing protocols, see our tirzepatide dosage chart. To understand fat loss mechanisms, see does tirzepatide burn fat. For long-term safety data, see tirzepatide long-term side effects.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
SURMOUNT-1 DEXA Body Composition Data: The Full Breakdown
The question "does tirzepatide cause muscle loss" remained poorly answered until February 2025, when Look et al. published the complete DEXA body composition substudy from SURMOUNT-1 in Diabetes, Obesity and Metabolism. This was not an estimate or an extrapolation. It was dual-energy X-ray absorptiometry on 160 participants, measuring fat and lean tissue separately at baseline and week 72 (Look et al., 2025).
The substudy enrolled 124 tirzepatide-treated participants and 36 on placebo. Mean baseline weight was 102.5 kg with a BMI of 38.0. The population was 73% female.
| Measurement | Tirzepatide (pooled doses) | Placebo |
|---|---|---|
| Total weight change | -21.3% | -5.3% |
| Fat mass change | -33.9% | -8.2% |
| Lean mass change | -10.9% | -2.6% |
| Absolute fat mass lost | 15.9 kg | 3.6 kg |
| Absolute lean mass lost | 5.6 kg | 1.2 kg |
| Proportion of weight lost as fat | 75% | 75% |
| Proportion of weight lost as lean | 25% | 25% |
Two findings from this substudy deserve attention. First, the 75/25 split held consistent across subgroups: men and women, younger and older participants, higher and lower baseline BMI. Second, placebo participants who lost weight through lifestyle changes alone showed the same 75/25 ratio. The drug did not worsen the lean mass loss beyond what caloric restriction itself produces.
What "Lean Mass" Actually Includes on a DEXA Scan
DEXA reports three compartments: fat mass, lean soft tissue, and bone mineral content. "Lean mass" is not purely skeletal muscle. It includes organ tissue, connective tissue, blood volume, and intracellular water bound to glycogen.
When you start tirzepatide, insulin sensitivity improves within the first 2 to 4 weeks. Glycogen stores in muscle and liver deplete, releasing bound water (each gram of glycogen holds 3 to 4 grams of water). A 90 kg person carries roughly 400 to 500 grams of glycogen, meaning 1.5 to 2 kg of the early "lean mass loss" on DEXA is water, not contractile muscle fiber.
The SURPASS-3 MRI substudy addressed this limitation by measuring thigh muscle volume and muscle fat infiltration directly. Published in The Lancet Diabetes & Endocrinology in June 2025, the analysis found that tirzepatide-treated participants showed reductions in muscle volume proportional to their weight loss, but muscle fat infiltration improved (Lancet Diabetes Endocrinol, 2025). The muscle that remained was leaner and higher quality than before treatment. Think of it like renovating a building: the square footage decreased, but the structural integrity per square foot improved.
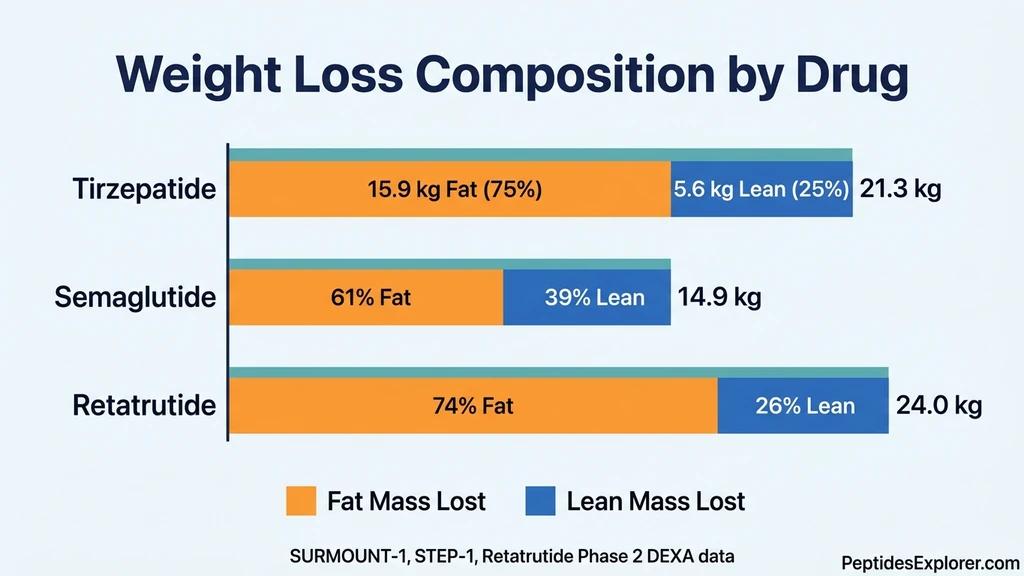
Tirzepatide vs Semaglutide vs Retatrutide: Muscle Loss Comparison
Not all GLP-1 drugs strip lean mass at the same rate. The fraction of weight lost as lean tissue varies significantly across molecules, and tirzepatide performs better than its closest competitor.
| Drug | Trial | Total Weight Loss | Lean Mass as % of Weight Lost | Absolute Lean Mass Lost | Fat-to-Lean Ratio |
|---|---|---|---|---|---|
| Tirzepatide 15 mg | SURMOUNT-1 DEXA | -21.3% | 25% | 5.6 kg | 3:1 |
| Semaglutide 2.4 mg | STEP 1 DEXA | -14.9% | 39% | 6.9 kg | 1.6:1 |
| Retatrutide 12 mg | Phase 2 DEXA | -24.0% | 26% | 6.2 kg | 2.8:1 |
| Diet alone (no drug) | Look-AHEAD | -8.6% | 25-33% | ~3.0 kg | 2:1 to 3:1 |
Sources: SURMOUNT-1 (Look et al., 2025); STEP 1 (Wilding et al., NEJM 2021); Retatrutide Phase 2 (Jastreboff et al., NEJM 2023); Look-AHEAD (Pownall et al., 2015).
Why Tirzepatide Preserves More Muscle Than Semaglutide
Semaglutide activates one receptor: GLP-1. Tirzepatide activates two: GLP-1 and GIP. That second receptor appears to matter for body composition.
GIP receptors are expressed on adipocytes, bone cells, and in the central nervous system. Activation of GIP signaling appears to improve adipocyte function and fat metabolism, which may direct the body to preferentially mobilize fat stores rather than catabolize muscle protein during energy deficit. A network meta-analysis of GLP-1 agonists and co-agonists found that tirzepatide achieved the largest fat mass reduction with the smallest proportional lean mass loss of any incretin-based therapy studied (ScienceDirect, 2024).
The SURMOUNT-5 trial confirmed tirzepatide's advantage in a head-to-head comparison. At 72 weeks, tirzepatide produced 20.2% weight loss versus 13.7% for semaglutide. Waist circumference dropped 18.4 cm with tirzepatide versus 13.0 cm with semaglutide, suggesting greater visceral fat loss rather than lean tissue depletion (Aronne et al., NEJM 2025).
Retatrutide: The Triple Agonist Comparison
Retatrutide adds a glucagon receptor to GLP-1 and GIP. The Phase 2 body composition substudy showed 26% of total weight lost was lean mass at the 12 mg dose, with absolute lean mass loss of approximately 6.2 kg (Lancet Diabetes Endocrinol, 2025). Despite producing the largest total weight loss (24% at 48 weeks), retatrutide preserved lean mass at a rate similar to tirzepatide.
The glucagon receptor drives hepatic thermogenesis, burning fat through liver metabolism rather than relying solely on reduced food intake. This additional fat-burning pathway may partially explain why lean mass loss stays proportionally low despite aggressive total weight loss. For dosing details, see our retatrutide dosage guide.
The Protein Protocol: How Much You Need to Protect Muscle
Protein is the non-negotiable foundation. Without adequate protein during caloric restriction, the body breaks down skeletal muscle to harvest amino acids for essential functions: immune defense, enzyme production, and organ maintenance. Your biceps are an amino acid savings account, and caloric deficit is a withdrawal notice.
A systematic review of protein requirements during weight loss found that intakes above 1.2 g/kg body weight consistently preserved lean mass compared to lower protein diets (Wycherley et al., Am J Clin Nutr, 2012). For GLP-1 users specifically, a 2025 Circulation review recommended 1.2 to 1.6 g/kg as the target range, noting that the upper end supports active individuals engaged in resistance training (Neeland et al., Circulation, 2024).
Protein Targets by Body Weight
| Body Weight | Minimum (1.2 g/kg) | Optimal (1.6 g/kg) | Daily Meals (4x) |
|---|---|---|---|
| 70 kg (154 lb) | 84 g | 112 g | 28 g per meal |
| 80 kg (176 lb) | 96 g | 128 g | 32 g per meal |
| 90 kg (198 lb) | 108 g | 144 g | 36 g per meal |
| 100 kg (220 lb) | 120 g | 160 g | 40 g per meal |
| 110 kg (242 lb) | 132 g | 176 g | 44 g per meal |
Use current body weight, not goal weight. As you lose weight, recalculate every 10 kg lost. The per-meal target matters because muscle protein synthesis saturates at approximately 25 to 40 grams per meal. Eating 100 grams at dinner and 10 grams at breakfast wastes the anabolic window. Spread intake across 3 to 4 meals with at least 25 grams each.
Practical Protein Sources When Appetite Is Suppressed
Tirzepatide reduces food intake by 20 to 35%. Many users struggle to hit protein targets because they simply are not hungry enough to eat. Calorie-efficient, protein-dense foods solve this problem.
| Food | Protein | Calories | Protein per 100 Calories |
|---|---|---|---|
| Whey protein isolate (1 scoop) | 27 g | 120 | 22.5 g |
| Nonfat Greek yogurt (1 cup) | 20 g | 100 | 20 g |
| Chicken breast (4 oz) | 35 g | 165 | 21 g |
| Egg whites (4 large) | 14 g | 68 | 21 g |
| Cottage cheese 1% (1 cup) | 28 g | 160 | 17.5 g |
| Canned tuna (1 can, drained) | 20 g | 90 | 22 g |
| Shrimp (4 oz) | 24 g | 100 | 24 g |
Whey protein isolate and shrimp deliver the highest protein per calorie. A morning shake (27 g), a lunch of chicken breast (35 g), an afternoon Greek yogurt (20 g), and a dinner with shrimp and cottage cheese (52 g) hits 134 grams at roughly 800 calories. That leaves 400 to 700 calories for vegetables, fats, and carbohydrates on a typical tirzepatide-restricted intake of 1,200 to 1,500 calories.
Resistance Training Protocol for GLP-1 Users
A 2025 Medscape review of resistance training combined with protein supplementation during GLP-1 therapy found that participants lost approximately 13% of body weight but only 3% of muscle mass, a dramatic improvement over the 10.9% lean mass decline seen in SURMOUNT-1 where exercise was not mandated (Medscape, 2025).
Muscle that is mechanically loaded sends a survival signal: this tissue is essential, do not break it down for fuel. Without that signal, the body treats skeletal muscle as an expendable energy reserve during caloric deficit.
Minimum Effective Dose: 2 Sessions Per Week
You do not need to train like a bodybuilder. Research on lean mass preservation during weight loss consistently shows that 2 sessions per week of compound resistance training preserves 50 to 80% more lean mass than no training at all.
Each session should include 4 to 5 compound movements that target large muscle groups. The load should be heavy enough that the final 2 to 3 repetitions of each set require genuine effort. If you can complete all reps easily, increase the weight by 5 to 10%.
Sample Session A (Lower Body Focus) 1. Barbell or goblet squat: 3 sets of 8 to 12 reps 2. Romanian deadlift: 3 sets of 8 to 10 reps 3. Walking lunges: 3 sets of 10 per leg 4. Leg press or leg curl: 3 sets of 10 to 12 reps 5. Standing calf raise: 3 sets of 12 to 15 reps
Sample Session B (Upper Body Focus) 1. Bench press or dumbbell press: 3 sets of 8 to 12 reps 2. Barbell row or cable row: 3 sets of 8 to 10 reps 3. Overhead press: 3 sets of 8 to 10 reps 4. Lat pulldown or pull-ups: 3 sets of 8 to 12 reps 5. Dumbbell curls / tricep pushdowns: 2 sets of 10 to 12 each
Training Adjustments for Tirzepatide Users
Reduced caloric intake means reduced recovery capacity. Three modifications prevent overtraining and injury during GLP-1 therapy.
First, reduce volume by 20 to 30% compared to your pre-treatment program. If you normally perform 16 sets per muscle group per week, drop to 10 to 12 sets. The stimulus for muscle preservation requires far less volume than the stimulus for muscle growth.
Second, prioritize compound movements over isolation exercises. A squat activates quadriceps, glutes, hamstrings, and core simultaneously. A leg extension activates only quadriceps. When energy is limited, compound movements deliver more preservation signal per calorie of recovery cost.
Third, schedule training sessions on days when appetite is highest. Many tirzepatide users report that appetite fluctuates throughout the week, with the day before injection and 2 to 3 days after injection being the lowest. Training when you can eat adequately afterward supports muscle repair and reduces soreness.
Supplements That Protect Lean Mass: Creatine, HMB, and Leucine
Three supplements have published evidence supporting lean mass preservation during caloric restriction. The strength of evidence varies. None replace protein and resistance training. They are additions to a foundation, not substitutes for it.
Creatine Monohydrate: Strong Evidence
Creatine is the most studied sports supplement in history. Meta-analyses in adults aged 50 to 80 show that creatine combined with resistance training increased lean body mass by an average of 1.32 kg compared to resistance training alone. In younger adults, the effect is larger: 1.5 to 2.0 kg over 8 to 12 weeks of training.
No study has tested creatine specifically in a GLP-1 agonist population. However, the mechanism is well understood. Creatine increases phosphocreatine stores in muscle, allowing more work per set, which amplifies the mechanical loading signal that preserves muscle. A 2025 narrative review on dietary supplements during GLP-1 therapy recommended daily creatine supplementation with resistance training as a reasonable addition to a muscle preservation plan (PMC, 2025).
Protocol: 3 to 5 grams of creatine monohydrate daily, taken with any meal. No loading phase required. Creatine pulls water into muscle cells, which may offset 1 to 2 kg of scale weight loss. This is intramuscular water, not fat. Do not adjust your tirzepatide dose based on a creatine-related scale stall.
HMB (Beta-Hydroxy Beta-Methylbutyrate): Moderate Evidence
HMB is a metabolite of the amino acid leucine. It inhibits muscle protein breakdown through two pathways: suppressing the ubiquitin-proteasome system and activating mTOR signaling. A meta-analysis found HMB supplementation significantly increased fat-free mass in older adults compared to placebo (Courel-Ibanez et al., 2019).
The International Society of Sports Nutrition position stand on HMB, updated in 2024, concluded that 3 g/day is warranted to support protein turnover pathways, particularly in populations experiencing caloric restriction or age-related muscle decline (JISSN, 2024). The benefits are most pronounced in untrained individuals and older adults, the same populations most vulnerable to muscle loss on GLP-1 agonists.
Protocol: 3 grams daily, split into three 1-gram doses with meals. HMB-FA (free acid form) absorbs faster than HMB-Ca (calcium salt). Both are effective. Expect modest effects: HMB is not creatine. It prevents breakdown rather than building new tissue.
Leucine: Supportive Evidence
Leucine is the amino acid that triggers muscle protein synthesis most potently. A threshold dose of approximately 2.5 to 3 grams of leucine per meal is required to maximally stimulate mTOR-mediated protein synthesis in skeletal muscle.
Whey protein naturally contains 10 to 11% leucine by weight, so a 27-gram scoop delivers approximately 2.7 to 3.0 grams of leucine. This is one reason whey protein consistently outperforms other protein sources for muscle preservation in clinical trials. If your protein source is plant-based (pea, rice, soy), leucine content is lower (6 to 8%), and supplementing an additional 1 to 2 grams of leucine per meal may be beneficial.
Protocol: Ensure each meal contains at least 2.5 grams of leucine. If using whey protein, this is built in. If using plant protein, add 1 to 2 grams of free-form leucine per serving.
Who Is at Highest Risk for Muscle Loss on Tirzepatide?
Not everyone faces equal risk. Four populations need aggressive muscle preservation strategies from day one of treatment.
Adults Over 50: Sarcopenia Compounds the Problem
After age 50, humans lose 1 to 2% of skeletal muscle mass per year through age-related sarcopenia. This is happening with or without tirzepatide. Adding a drug that creates a 500 to 750 calorie daily deficit accelerates an already active process.
A 55-year-old woman weighing 95 kg with baseline low muscle mass could lose 5 to 6 kg of lean tissue over 72 weeks on tirzepatide. If she started with borderline-low grip strength (below the 25th percentile for her age), that loss could push her into clinical sarcopenia: difficulty climbing stairs, increased fall risk, and reduced independence.
The fix is prevention, not reaction. Start resistance training and protein supplementation before or simultaneously with tirzepatide initiation. Baseline DEXA and grip strength measurement provide a reference point. Repeat DEXA at 6 and 12 months. If lean mass drops more than 5% while fat mass is declining appropriately, increase protein and training intensity before increasing the tirzepatide dose.
Users Eating Below 1,000 Calories Daily
Some users on tirzepatide 10 or 15 mg eat 800 to 1,000 calories daily because the appetite suppression is that powerful. At these caloric levels, even with perfect protein distribution, the body cannot maintain muscle mass. The energy deficit is too severe.
A 90 kg person on 900 calories needs approximately 108 grams of protein (1.2 g/kg). That is 432 protein calories, leaving 468 calories for everything else: fats, carbohydrates, vitamins, minerals, fiber. It is nearly impossible to meet micronutrient needs at this level while preserving muscle.
If your daily intake consistently falls below 1,000 calories, discuss dose reduction with your prescriber. SURMOUNT-1 showed that 10 mg produced 21.4% weight loss versus 22.5% at 15 mg. That 1.1 percentage point difference may not justify the additional appetite suppression that pushes caloric intake into a dangerous zone. Use our tirzepatide dosage calculator to review titration options.
Sedentary Individuals with No Training History
If you have never performed resistance training, your muscles have no recent adaptation signal telling the body they are essential. During caloric restriction, trained muscle is preserved at a higher rate than untrained muscle because the mechanical loading creates a molecular signal (through mTOR and other pathways) that flags the tissue as functionally important.
Starting a basic resistance program, even bodyweight exercises like wall push-ups, chair squats, and resistance band rows, sends that preservation signal. A 2025 case series of GLP-1 users who combined their medication with supervised resistance training and adequate protein showed that lean soft tissue loss comprised only 3 to 8% of total weight lost, far below the 25% observed in the SURMOUNT-1 DEXA substudy (PMC, 2025).
Monitoring Muscle Loss: DEXA Scans, Grip Strength, and Functional Tests
The scale tells you nothing about muscle. You need direct measurements.
DEXA Scans: The Gold Standard
Dual-energy X-ray absorptiometry separates your body into three compartments: fat mass, lean soft tissue, and bone mineral content. A baseline scan before starting tirzepatide and follow-up scans at 6 and 12 months provide objective data on whether your muscle preservation protocol is working.
Cost ranges from $75 to $200 per scan depending on location. Many obesity medicine clinics now offer DEXA as part of GLP-1 treatment monitoring. Request the appendicular lean mass index (ALMI), which divides lean mass in the arms and legs by height squared. An ALMI below 7.0 kg/m2 in men or 5.5 kg/m2 in women indicates sarcopenia risk.
Grip Strength: A 30-Second Proxy
Grip strength correlates with total body muscle function and predicts mortality risk independently of other factors. A handheld dynamometer costs $25 to $40 and provides a reliable home measurement.
Measure three times with each hand, take the best score. Men below 26 kg and women below 18 kg meet the threshold for probable sarcopenia according to the European Working Group on Sarcopenia in Older People (EWGSOP2). Track monthly during tirzepatide treatment. A decline of more than 10% from baseline warrants reassessment of your protein intake and training program.
Functional Tests You Can Do at Home
Two simple tests track real-world muscle function without equipment.
Chair stand test: Sit in a standard-height chair with arms crossed. Stand up and sit down 5 times as fast as possible. Time yourself. Healthy adults under 60 complete this in under 11 seconds. Over 15 seconds suggests meaningful lower body strength loss.
Stair climb test: Climb 10 standard stairs as quickly and safely as possible. Time yourself at baseline and monthly. An increase of more than 3 seconds from baseline indicates declining lower extremity power.
These tests detect functional decline that DEXA alone may miss. A person can maintain lean mass on DEXA while losing functional strength if the remaining muscle has increased fat infiltration. The SURPASS-3 MRI substudy found that muscle fat infiltration improved with tirzepatide treatment, which is a positive signal for muscle quality even as total volume decreases (Lancet Diabetes Endocrinol, 2025).
What Happens If You Lose Too Much Muscle: A Clinical Scenario
A 58-year-old man started tirzepatide at 107 kg. He did no resistance training. He ate 1,100 calories daily with 50 grams of protein. By month 9, he had lost 25 kg of total body weight. His DEXA at month 10 showed 8.5 kg of lean mass loss alongside 16.5 kg of fat mass loss. That ratio, 1.9:1, was far worse than the 3:1 average from SURMOUNT-1.
The consequences were measurable. His resting metabolic rate dropped by an estimated 425 calories per day. His grip strength fell from the 35th to the 10th percentile for his age. He reported difficulty carrying groceries upstairs and fatigue during routine activities. His ALMI dropped to 6.8 kg/m2, placing him in the sarcopenia risk category.
His endocrinologist held the dose at 10 mg, prescribed 3 supervised resistance training sessions per week, and increased protein to 140 grams daily (1.6 g/kg of his reduced weight of 82 kg). Creatine at 5 grams daily was added. Over 4 months, a follow-up DEXA showed he had regained 2.5 kg of lean mass while continuing to lose 3 kg of fat. His grip strength improved to the 30th percentile.
This scenario is preventable. The muscle loss was not caused by tirzepatide's pharmacology. It was caused by inadequate protein (50 g versus the 128 g minimum at 1.2 g/kg), zero mechanical loading, and aggressive caloric restriction. The drug created the deficit. The missing protein and training created the muscle loss.
Important Safety Information
Tirzepatide is a prescription medication approved for type 2 diabetes (Mounjaro) and obesity (Zepbound). It is not approved for body recomposition or muscle preservation in normal-weight individuals.
Do not reduce prescribed protein intake to accelerate weight loss. Lean mass loss at rates exceeding 1% per month increases the risk of metabolic adaptation (reduced resting metabolic rate), falls and fractures in older adults, immune dysfunction, and poor wound healing. Report unexplained weakness, difficulty with daily activities, or significant grip strength decline to your prescriber.
Do not combine tirzepatide with other GLP-1 receptor agonists. Individuals with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not use tirzepatide. The drug carries a boxed warning for thyroid C-cell tumors based on rodent studies.
For injection technique and reconstitution guidance, see our dedicated guides. For monitoring other side effects, see our guides on headaches, constipation, and hair loss.
This article is educational content for research purposes. Consult a healthcare provider before starting, adjusting, or discontinuing any medication.
Frequently Asked Questions
How much muscle do you lose on tirzepatide?
SURMOUNT-1 DEXA data showed 5.6 kg (12.3 lb) of lean mass lost over 72 weeks, representing 25% of total weight lost. The remaining 75% (15.9 kg) was fat mass. With resistance training and protein intake above 1.2 g/kg, lean mass loss can be reduced to 3 to 8% of total weight lost based on case series data.
Is tirzepatide muscle loss worse than semaglutide?
No. Tirzepatide preserves more lean mass proportionally. SURMOUNT-1 showed 25% of weight lost was lean mass, while STEP 1 showed 39% for semaglutide 2.4 mg. The GIP receptor in tirzepatide may direct the body to preferentially mobilize fat stores, resulting in a 3:1 fat-to-lean ratio versus 1.6:1 for semaglutide.
Can you build muscle while taking tirzepatide?
Building new muscle during active weight loss is difficult because muscle growth requires a caloric surplus. However, you can preserve existing muscle and potentially regain lost mass once weight stabilizes. The SURPASS-3 MRI substudy showed muscle quality (reduced fat infiltration) improved even as total volume decreased, suggesting functional capacity can improve during treatment.
How much protein should I eat on tirzepatide to prevent muscle loss?
Aim for 1.2 to 1.6 grams of protein per kilogram of current body weight daily. For a 90 kg (198 lb) person, that means 108 to 144 grams spread across 3 to 4 meals of at least 25 grams each. Whey protein isolate delivers the highest protein per calorie (27 g per 120 calories) when appetite is suppressed.
Does creatine help prevent muscle loss on GLP-1 medications?
No study has tested creatine specifically in GLP-1 users. However, meta-analyses show creatine with resistance training adds an average of 1.32 kg lean body mass versus training alone in adults over 50. A 2025 review recommended daily creatine supplementation as a reasonable addition to a GLP-1 muscle preservation plan. The dose is 3 to 5 grams daily.
Should I get a DEXA scan while on tirzepatide?
A baseline DEXA before starting tirzepatide and follow-ups at 6 and 12 months provide objective body composition tracking. DEXA costs $75 to $200 per scan. Request the appendicular lean mass index (ALMI). An ALMI below 7.0 kg/m2 in men or 5.5 kg/m2 in women indicates sarcopenia risk requiring more aggressive protein and training intervention.
Does tirzepatide cause sarcopenia?
Tirzepatide does not directly cause sarcopenia (pathological muscle loss). However, the caloric deficit it creates can accelerate sarcopenia in at-risk populations: adults over 50, those with low baseline muscle mass, and sedentary individuals eating below 1,000 calories daily. Resistance training 2 to 3 times weekly and protein above 1.2 g/kg are the primary prevention strategies.
What is the fat-to-lean loss ratio on tirzepatide?
The SURMOUNT-1 DEXA substudy found a 3:1 fat-to-lean ratio (75% fat, 25% lean mass). This is better than semaglutide (1.6:1) and comparable to retatrutide (2.8:1). With structured resistance training and adequate protein, case series show the ratio can improve to 10:1 or better, with lean mass loss dropping to 3 to 8% of total weight lost.
The Bottom Line
Tirzepatide causes lean mass loss. The SURMOUNT-1 DEXA substudy quantified it: 5.6 kg over 72 weeks, representing 25% of total weight lost. That ratio is better than semaglutide (39% lean mass) and consistent with caloric restriction in general. The drug is not uniquely destructive to muscle. It creates a deficit, and deficits cost lean tissue unless you intervene.
The intervention is straightforward. Protein at 1.2 to 1.6 g/kg daily, resistance training 2 to 3 times per week, and creatine at 3 to 5 grams daily. These three measures can reduce lean mass loss from 25% to under 10% of total weight lost. A DEXA scan at baseline and 6 months tracks whether your protocol is working.
Use our tirzepatide dosage calculator to plan titration. For dose conversion details, see the tirzepatide dosage chart in units. For understanding how tirzepatide drives fat loss specifically, see does tirzepatide burn fat.
Related articles: - Tirzepatide Long-Term Side Effects - 72-week safety data including body composition changes - Does Tirzepatide Burn Fat? - fat loss mechanisms and body composition analysis - Retatrutide vs Tirzepatide - head-to-head comparison of weight loss peptides - Peptide Safety Guide - comprehensive safety information for all peptides - How to Inject Tirzepatide - injection technique for optimal absorption - Not Losing Weight on Semaglutide - troubleshooting GLP-1 weight loss stalls
Explore all peptide profiles and tools at PeptidesExplorer.
Helpful Tools
Related Articles
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
Does Tirzepatide Affect Your Period?
Does tirzepatide affect your period? Yes, via rapid fat loss and estrogen shifts. Cycle changes, PCOS fertility, and birth control warning.
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.
Can Tirzepatide Cause Anxiety?
Anxiety is reported in 3-6% of tirzepatide users. Learn SURMOUNT/SURPASS data, GLP-1 brain mechanisms, and 7 management strategies.