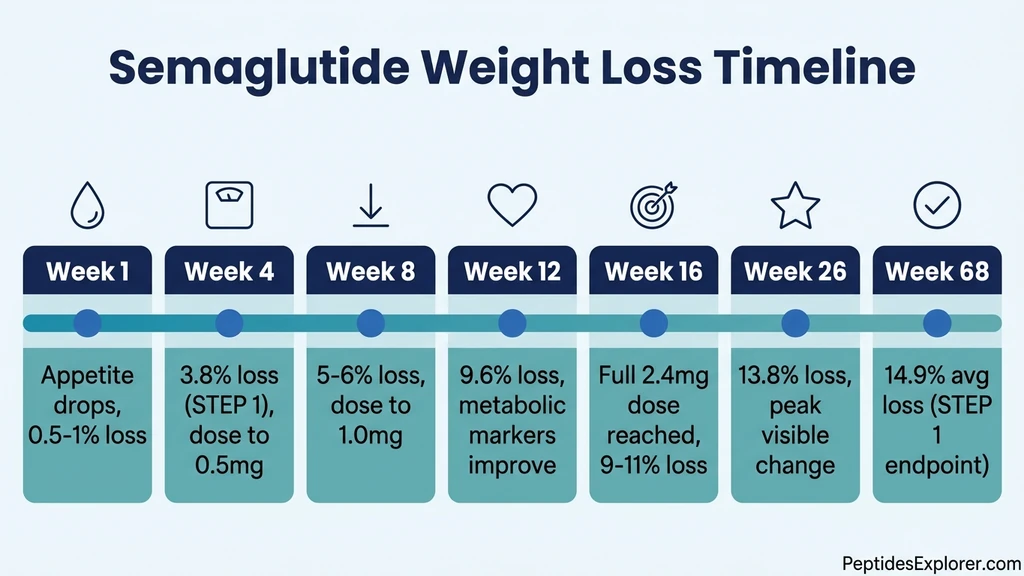
You filled your first semaglutide prescription and want to know when it starts working. Semaglutide suppresses appetite within the first week, produces measurable weight loss by week 4, and delivers 10-15% total body weight reduction by month 6. The STEP 1 clinical trial documented an average 3.8% body weight loss at week 4 and 14.9% at week 68 with the 2.4 mg dose (Wilding et al., NEJM 2021). But "working" depends on what you are measuring. Appetite control happens fast. The scale moves slower. Metabolic improvements unfold over months.
This article breaks down the full timeline so you know exactly what to expect each week, what clinical trial data actually shows, and what to do if your results fall behind the curve.
| Timeline | What Happens | Average Weight Loss | Key Milestone |
|---|---|---|---|
| Week 1 | Appetite drops, food noise quiets | 0.5-1% | First noticeable appetite change |
| Week 2-3 | Portions shrink naturally, cravings fade | 1-2% | Eating 20-30% fewer calories |
| Week 4 | First dose increase (0.25 to 0.5 mg) | 3-4% | First measurable scale change |
| Week 8 | Dose at 1.0 mg, consistent weekly loss | 5-6% | Clothes fit differently |
| Week 12 | Dose at 1.7 mg, metabolic markers shift | 7-9% | Blood sugar and triglycerides improve |
| Week 16 | Target dose of 2.4 mg reached | 9-11% | Peak rate of weekly loss |
| Week 24 | Six months, rate begins to slow | 12-14% | Most visible transformation |
| Week 68 | Trial endpoint | 14.9% (STEP 1 avg) | Weight loss plateaus near maximum |
Use our semaglutide dosage calculator to see the exact dose schedule and injection volumes for each escalation step.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How GLP-1 Receptor Agonists Work: The Thermostat Analogy
Think of your appetite as a thermostat set too high. Your brain's hypothalamus has a "set point" for body weight, and it defends that point aggressively. When you cut calories through willpower alone, your brain cranks up hunger hormones (ghrelin) and slows your metabolism. You fight the thermostat, and the thermostat usually wins.
Semaglutide turns the thermostat down. It mimics a natural hormone called GLP-1 (glucagon-like peptide-1) that your gut releases after eating. Natural GLP-1 survives in your bloodstream for about 2 minutes before enzymes break it down. Semaglutide is engineered to resist that breakdown, giving it a half-life of approximately 7 days (Marbury et al., 2017). One weekly injection maintains steady GLP-1 receptor activation that your body could never sustain on its own.
This sustained activation does three things simultaneously. First, it signals the hypothalamus to reduce hunger and increase satiety after smaller meals. Second, it slows gastric emptying so food stays in your stomach longer, extending the feeling of fullness. Third, it improves insulin sensitivity and reduces glucagon secretion, stabilizing blood sugar swings that trigger cravings. The SUSTAIN trial program confirmed these effects in patients with type 2 diabetes, showing significant HbA1c reductions alongside weight loss (Sorli et al., 2017).
The thermostat analogy explains why semaglutide works differently from dieting. You are not fighting your appetite. The drug resets the signal that creates your appetite. That is why users describe the experience as "food noise disappearing" rather than "resisting cravings." The subjective experience of hunger genuinely changes.
Week 1: Appetite Suppression Begins
Semaglutide reaches therapeutic blood levels within 24-72 hours of the first injection. The starting dose of 0.25 mg is intentionally low to let your GI tract adjust, but it is already active at the receptor level.
Most users notice the first change within 3-5 days: reduced interest in food between meals. The internal monologue about what to eat next goes quiet. A clinical pharmacology study on oral semaglutide found that ad libitum energy intake decreased by 38.9% compared to placebo, driven primarily by reduced appetite and lower preference for high-fat foods (Blundell et al., 2020). While this study used the oral formulation at higher doses, the underlying mechanism is identical for injectable semaglutide.
What to expect in week 1: - Appetite noticeably lower by day 3-5 - You may forget to eat a meal (this is a common early sign it is working) - Portion sizes naturally shrink by 15-25% - Scale may show 0.5-1 lb loss (mostly from reduced food volume, not fat loss yet) - Mild nausea is possible but not universal (about 20% of users at 0.25 mg)
If nausea appears, it typically peaks 24-48 hours after injection and fades by day 4. This is the drug slowing gastric emptying, not a sign of a problem. Eating smaller, blander meals during the first 48 hours after injection helps significantly.
What week 1 does not look like: Dramatic weight loss, zero appetite, or feeling sick all day. The 0.25 mg dose is a warm-up. Real momentum builds over the next several weeks as doses increase.
Weeks 2-4: The First Measurable Changes
By the second injection, semaglutide blood levels are climbing toward steady state. GLP-1 receptor activation in the hypothalamus deepens. Users report that the appetite suppression from week 1 becomes more consistent and predictable.
The STEP 1 trial measured weight at week 4 and found an average loss of 3.8% of baseline body weight in the semaglutide group versus 1.3% in the placebo group (Wilding et al., 2021). For a 220 lb (100 kg) starting weight, that translates to roughly 8.4 lbs lost in the first month. That number includes participants still on the 0.25 mg starting dose and those who had just increased to 0.5 mg at week 4.
Week 2: Cravings Fade
The second week is when most users notice cravings weaken. Sugar cravings, late-night snacking urges, and the pull toward high-calorie comfort foods all diminish. Research shows semaglutide specifically reduces preference for energy-dense, fatty foods (Blundell et al., 2020). This is not willpower. The drug changes what your brain finds rewarding about food.
Practical signs it is working: - You leave food on your plate without trying - Fast food and junk food lose their appeal - You eat because it is mealtime, not because you are driven to eat - Caloric intake drops by 20-35% without conscious restriction
For users with type 2 diabetes, blood sugar may already begin to stabilize. The SUSTAIN 1 trial showed significant fasting glucose reductions as early as week 4 (Sorli et al., 2017).
Week 3-4: The Scale Moves
Weeks 3-4 are when the scale starts reflecting real fat loss, not just reduced food volume. At the standard dosage schedule, you increase from 0.25 mg to 0.5 mg at week 4. This dose escalation amplifies both appetite suppression and metabolic effects.
What the data shows at week 4: - STEP 1: Average 3.8% body weight loss (semaglutide 2.4 mg group, including titration) - 86.4% of participants had lost at least some weight - Waist circumference began decreasing - Systolic blood pressure dropped by 2-3 mmHg on average
If you have not lost anything by week 4, do not panic. Individual responses vary. Some users see little scale movement in the first month but accelerate in months 2-3 as doses increase. If the scale has not moved by week 8, read our guide on not losing weight on semaglutide for troubleshooting steps.
Months 2-3: Rapid Weight Loss Phase
Months 2 and 3 represent the steepest part of the weight loss curve. You are escalating through the middle dose range (0.5 mg to 1.0 mg to 1.7 mg), and each increase deepens the appetite and metabolic effects. The body has adapted to semaglutide enough that GI side effects typically diminish, but the weight loss mechanism is running at full speed.
The STEP 1 trial recorded an average of 9.6% body weight loss at week 12 in the semaglutide group (Wilding et al., 2021). For a 220 lb starting weight, that is approximately 21 lbs lost by the three-month mark. The rate during this phase works out to roughly 1-2% body weight per month, or 2-4 lbs per week for most users.
Month 2 (Weeks 5-8): Building Momentum
At week 5 you are on 0.5 mg. At week 8 you increase to 1.0 mg. This is the dose range where many users describe a "switch flipping." The difference between 0.25 mg and 1.0 mg is substantial.
What changes in month 2: - Hunger signals become genuinely faint between meals - Meal sizes shrink to 50-60% of pre-treatment portions - Energy levels may temporarily dip as caloric intake drops (read about semaglutide and fatigue if this happens) - Fat loss becomes visible in the face, neck, and midsection - Clothes that were tight begin to fit loosely
Some users report that the 0.5 mg to 1.0 mg jump at week 8 causes a brief return of nausea. This is expected. Your GI tract is adjusting to a stronger dose. The nausea resolves within 5-10 days for most people. If it persists, learn how to relieve nausea from semaglutide.
Month 3 (Weeks 9-12): Metabolic Improvement
By month 3, semaglutide is producing effects beyond the scale. Blood work often shows measurable improvements in metabolic markers.
Clinical trial data at 12 weeks: - Average total weight loss: 9.6% (STEP 1) - HbA1c reduction: 1.0-1.5 percentage points in patients with diabetes (SUSTAIN trials) - Triglycerides: 10-15% lower - LDL cholesterol: modest improvement - Systolic blood pressure: 3-5 mmHg lower - Waist circumference: reduced by 4-6 cm on average
The metabolic improvements matter because they reduce cardiovascular risk independently of weight loss. The SELECT trial (semaglutide 2.4 mg in patients with obesity and cardiovascular disease) showed a 20% reduction in major adverse cardiovascular events (Lincoff et al., NEJM 2023). This benefit began emerging within the first 6 months.
Month 3 is also when semaglutide before and after photos start showing clear differences. The face is usually the first place where others notice the change.
Months 4-6: Peak Weight Loss and Target Dose
You reach the full 2.4 mg target dose at week 16 (month 4). From months 4 through 6, you are at maximum dose with full receptor saturation. The rate of weight loss peaks during this period, then begins to decelerate as the body approaches a new equilibrium.
The STEP 1 trial recorded an average of 13.8% body weight loss at week 26 (6 months) in the semaglutide group versus 3.7% in the placebo group. That gap (10.1 percentage points attributable to the drug) represents the core pharmacological effect at the six-month mark. For a 220 lb starting weight, 13.8% loss translates to roughly 30 lbs.
Month 4 (Weeks 13-16): Reaching Full Dose
The standard titration schedule moves from 1.0 mg (week 8) to 1.7 mg (week 12) and finally to 2.4 mg (week 16). Each increase provides incrementally stronger appetite suppression.
What to expect at full dose: - Appetite suppression reaches maximum intensity - Some users feel they have to remind themselves to eat - Caloric intake is typically 30-40% below pre-treatment levels - Weekly weight loss of 1-2 lbs continues steadily - GI side effects have usually resolved by this point
If GI side effects return at 1.7 mg or 2.4 mg, your prescriber may slow the escalation or keep you at a lower dose. Read our guide on how to microdose semaglutide to understand lower-dose maintenance options. Weight loss still occurs at lower doses, just at a slower rate.
Months 5-6 (Weeks 17-26): The Visible Transformation
This period produces the most dramatic visual changes. By now you have lost 25-35 lbs on average (for someone starting at 220 lbs). Friends and coworkers who have not seen you in a few months will comment. Wardrobe changes become necessary.
Physical changes at the 6-month mark: - Face, jawline, and neck visibly thinner - Midsection significantly reduced - Waist circumference down 5-8 cm on average - Energy and mobility improved - Blood pressure often normalized - Sleep quality improved (less weight on the diaphragm, reduced sleep apnea symptoms)
The rate of loss begins to slow during months 5-6. This is not a plateau. It is the mathematical consequence of weighing less: a body that weighs 190 lbs burns fewer calories at rest than a body that weighs 220 lbs. The caloric deficit narrows naturally as you lose weight. In the STEP 1 trial, the weight loss curve flattened visibly after week 30.
If you are considering switching to tirzepatide for additional weight loss, our semaglutide to tirzepatide switching guide covers the conversion protocol.
Months 7-17: Maintenance and Long-Term Results
The STEP 1 trial ran for 68 weeks (approximately 17 months). Weight loss continued to accrue after month 6 but at a progressively slower rate. The curve reached a nadir (lowest point) around week 60, with a final average loss of 14.9% body weight.
What the long-term data shows: - Week 26 to week 68: approximately 1-2% additional body weight loss (the pace slows dramatically) - 86.4% of participants lost at least 5% body weight - 69.1% lost at least 10% - 50.5% lost at least 15% - 32.0% lost at least 20%
These numbers mean that roughly one-third of users on the full 2.4 mg dose lose 20% or more of their starting weight. For a 220 lb person, that is 44+ lbs. The other two-thirds still lose meaningful amounts, but the distribution of individual responses is wide.
The weight regain question: The STEP 1 trial extension followed participants who stopped semaglutide at week 68. Within one year of stopping, they regained two-thirds of the weight they had lost (Wilding et al., 2022). This finding confirmed that semaglutide suppresses weight through ongoing pharmacological action, not permanent metabolic reprogramming. For most users, semaglutide stays in your system for about 5 weeks after the last injection before its effects fully fade. Continued treatment is necessary to maintain the results.
Factors That Affect How Fast Semaglutide Works
The STEP trials report averages, but individual responses vary widely. Some users lose 25% of their body weight, others lose 5%. Four factors explain most of this variation.
Dose and Titration Speed
Higher doses produce more weight loss. The STEP 2 trial compared 1.0 mg versus 2.4 mg in patients with type 2 diabetes and found a clear dose-response: 7.0% versus 9.6% weight loss at 68 weeks (Davies et al., 2021). Users who cannot tolerate the 2.4 mg dose still lose weight at 1.0 mg or 1.7 mg, just less and slower.
The titration speed also matters. The standard 4-week escalation schedule gets you to 2.4 mg by week 16. If GI side effects force a slower escalation (6-8 weeks per step), you reach full dose later and the maximum weight loss trajectory shifts by 4-8 weeks. This delay does not reduce the final outcome. It just takes longer to get there.
Check your exact dose volume and concentration with the semaglutide dosage calculator.
Diet and Caloric Deficit
Semaglutide reduces appetite, but it does not force a specific caloric deficit. Users who eat high-calorie, nutrient-poor foods can still overconsume, especially calorie-dense liquids (smoothies, alcohol, sugary coffee drinks) that bypass the gastric emptying delay.
The STEP trials included lifestyle counseling. Participants ate a reduced-calorie diet (approximately 500 kcal below estimated needs) and exercised 150 minutes per week. In real-world practice, many users do not follow structured diets, and their results fall below the trial averages.
The compounding effect: Pairing semaglutide with a protein-rich diet (0.8-1.0 g protein per lb of lean body mass) preserves muscle mass during weight loss. Muscle preservation keeps metabolic rate higher, which sustains the caloric deficit longer. Users who eat adequate protein consistently outperform those who eat whatever they want in reduced portions.
If you are using compound semaglutide with B12, the added vitamin B12 may help with energy levels during the caloric deficit but does not directly accelerate fat loss.
Exercise and Physical Activity
Exercise amplifies semaglutide's effects through two mechanisms. First, it increases the caloric deficit beyond what appetite suppression alone achieves. Second, resistance training preserves lean muscle mass during rapid weight loss, preventing the metabolic slowdown that blunts long-term results.
A 2024 study combined semaglutide with a supervised exercise program and found that the combination group lost significantly more fat mass while preserving more lean mass compared to semaglutide alone (Lundgren et al., NEJM 2024). The exercise did not need to be extreme. Walking 150 minutes per week plus 2-3 resistance training sessions was the protocol.
Practical takeaway: Semaglutide does the heavy lifting on appetite. Exercise shapes what kind of weight you lose (fat vs. muscle). Both matter.
Starting Weight and Metabolic Health
Users with higher starting BMIs tend to lose more absolute weight but a similar percentage of body weight. A 300 lb person losing 15% drops 45 lbs. A 200 lb person losing 15% drops 30 lbs. Both achieved the same pharmacological effect.
Metabolic health also matters. Users with type 2 diabetes typically lose less weight on semaglutide than users without diabetes. The STEP 2 trial (all participants had type 2 diabetes) showed 9.6% weight loss at 68 weeks with 2.4 mg, compared to 14.9% in STEP 1 (no diabetes requirement). Insulin resistance appears to blunt the weight loss response, though blood sugar improvements are excellent.
Users who have tried and failed multiple diets, suggesting strong metabolic adaptation, may respond slower initially but still achieve clinically meaningful weight loss by month 6.
What to Do If Semaglutide Is Not Working
"Not working" usually means one of three things: the scale has not moved, you do not feel appetite suppression, or results plateaued earlier than expected. Each has a different solution.
The Scale Has Not Moved After 4-6 Weeks
First, confirm you are actually on the correct dose and injecting properly. Subcutaneous injection technique matters. If the drug leaks or is injected intradermally instead of subcutaneously, absorption changes. Verify your injection volume against the semaglutide dosage chart in mL.
Second, track your food intake for one week. Semaglutide reduces appetite, but liquid calories (alcohol, sugary drinks, calorie-dense smoothies) often bypass the satiety mechanism. Users who drink 500+ calories per day in liquids may not achieve a sufficient caloric deficit despite reduced solid food intake.
Third, check if you are on branded or compounded semaglutide. Compounded versions vary in quality. If your semaglutide looks red or discolored, it may have degraded. Ensure proper refrigeration and storage.
Our full troubleshooting guide covers all scenarios: not losing weight on semaglutide.
You Do Not Feel Appetite Suppression
Some users at 0.25 mg or 0.5 mg report minimal appetite change. This is normal. The lower doses are titration steps, not therapeutic doses. The STEP trials used 2.4 mg as the treatment dose because lower doses showed less appetite suppression and weight loss in dose-finding studies.
If you still feel no appetite change at 1.0 mg or above, discuss with your prescriber. Possible explanations include: a genetic variant in the GLP-1 receptor that reduces sensitivity (rare but documented), medication interactions that affect absorption, or emotional/behavioral eating patterns that semaglutide does not address. Semaglutide targets physiological hunger. It does not eliminate stress eating, boredom eating, or eating from habit.
Approximately 10-15% of users are classified as "non-responders" in clinical trials. If you have reached 2.4 mg with adequate titration time and still see no results, tirzepatide is the usual next step. It adds GIP receptor activation to GLP-1, and some semaglutide non-responders respond well to the dual agonist.
Results Plateaued Earlier Than Expected
Weight loss plateaus are mathematically inevitable. As you lose weight, your body requires fewer calories to maintain its smaller mass. The caloric deficit shrinks even if you eat the same amount. True plateaus (no weight loss for 4+ consecutive weeks at full dose) deserve investigation.
Common causes of early plateaus: - Unconscious calorie creep: portions gradually increasing as you adjust to the medication - Reduced physical activity: feeling less energetic on a sustained caloric deficit - Fluid retention masking fat loss (especially in women during certain menstrual cycle phases) - Metabolic adaptation: your body becomes more efficient at lower weight
Solutions: 1. Recalculate your caloric needs at your new weight 2. Add or intensify resistance training 3. Ensure protein intake is adequate (prevents muscle loss that slows metabolism) 4. Ask your prescriber about temporarily increasing the dose if you are below 2.4 mg 5. Consider that you may have reached a new set point that requires additional interventions
Some users cycle off semaglutide for 4-6 weeks and restart to "reset" responsiveness. The evidence for this strategy is anecdotal. Given that semaglutide has a long half-life and stays in your system for weeks, the washout period needs to be at least 5 weeks for full clearance.
Common Mistakes That Slow Your Results
Four mistakes account for most cases where semaglutide works slower than clinical trial averages suggest.
Mistake 1: Expecting visible results in week 1. Semaglutide starts working immediately at the receptor level, but visible weight loss takes 3-4 weeks. The first week is primarily appetite changes and reduced food volume. Fat loss is a slower process. Users who step on the scale daily during weeks 1-2 and see fluctuations often panic unnecessarily. Weigh yourself once per week, same day, same time, same conditions.
Mistake 2: Not increasing the dose on schedule. The 0.25 mg starting dose is not a treatment dose. It is a GI tolerance dose. Users who stay at 0.25 mg or 0.5 mg for months because they "feel fine" are leaving significant weight loss on the table. The dose-response data from STEP 2 is clear: 2.4 mg produces more weight loss than 1.0 mg (Davies et al., 2021). Follow the escalation schedule unless side effects prevent it.
Mistake 3: Drinking calories. Semaglutide slows gastric emptying and reduces appetite for solid food. Liquids empty from the stomach faster and do not trigger the same satiety signals. A daily 400-calorie Starbucks drink, two glasses of wine, or a large smoothie can erase most of the caloric deficit that semaglutide creates. Users who eliminate liquid calories consistently outperform those who do not.
Mistake 4: Ignoring protein intake. Rapid weight loss on semaglutide includes muscle loss unless you actively prevent it. Muscle is metabolically expensive tissue. Losing it reduces your basal metabolic rate, which slows future weight loss. Aim for 0.7-1.0 g of protein per pound of target body weight per day. Prioritize protein at every meal. This single dietary change produces faster fat loss, better body composition, and a higher likelihood of maintaining results long-term.
Semaglutide for Diabetes vs. Weight Loss: Different Timelines
Semaglutide is FDA-approved under two brand names with different indications. Ozempic (0.25 mg, 0.5 mg, 1.0 mg, 2.0 mg) treats type 2 diabetes. Wegovy (0.25 mg, 0.5 mg, 1.0 mg, 1.7 mg, 2.4 mg) treats obesity. The molecule is identical. The target doses and expected timelines differ.
For blood sugar control (diabetes indication): - HbA1c improvement begins within 4 weeks - Clinically significant HbA1c reduction (1.0-1.5 percentage points) by week 12-16 - The SUSTAIN 1 trial showed a 1.55% HbA1c reduction at week 30 with 1.0 mg semaglutide (Sorli et al., 2017) - Blood sugar control continues to improve through week 30 and stabilizes - Fasting glucose and postprandial glucose both decrease
For weight loss (obesity indication): - Appetite suppression within week 1 - Measurable weight loss by week 4 - Maximum rate of loss during months 2-4 - Average 14.9% loss at week 68 with 2.4 mg (STEP 1) - Weight loss curve flattens after month 6
The key difference: diabetes patients on Ozempic typically max out at 1.0-2.0 mg and achieve 5-7% weight loss. Obesity patients on Wegovy escalate to 2.4 mg and achieve 12-15%. The higher dose drives the additional weight loss. If you are using Ozempic for weight management and not reaching your goals, ask your prescriber about switching to the Wegovy dose schedule.
For details on how long semaglutide side effects last at each dose level, see our full side effects timeline guide.
How Semaglutide Speed Compares to Other GLP-1 Medications
Semaglutide is not the only GLP-1 receptor agonist. Understanding how it compares helps set realistic expectations.
| Medication | Mechanism | Avg Weight Loss (Trial Duration) | Time to See Results |
|---|---|---|---|
| Semaglutide 2.4 mg (Wegovy) | GLP-1 agonist | 14.9% (68 weeks, STEP 1) | 2-4 weeks |
| Tirzepatide 15 mg (Zepbound) | GLP-1 + GIP agonist | 22.5% (72 weeks, SURMOUNT-1) | 2-4 weeks |
| Liraglutide 3.0 mg (Saxenda) | GLP-1 agonist (daily) | 8.0% (56 weeks, SCALE) | 2-4 weeks |
| Retatrutide 12 mg | GLP-1 + GIP + glucagon agonist | 24.2% (48 weeks, Phase 2) | 2-4 weeks |
All GLP-1 medications begin suppressing appetite within the first week. The differences show up in the magnitude of weight loss over time, not in how quickly the initial effects appear. Tirzepatide produces roughly 50% more weight loss than semaglutide at maximum doses, primarily through the added GIP receptor activation. For users who started on semaglutide and want to try tirzepatide, the switching guide covers the dose conversion.
The timeline for how long semaglutide takes to work varies slightly depending on individual metabolism, but the first-week appetite changes are nearly universal across all GLP-1 medications.
Frequently Asked Questions
How fast does semaglutide suppress appetite?
Most users notice reduced appetite within 3-5 days of the first injection. The 0.25 mg starting dose is already active at GLP-1 receptors in the hypothalamus. Appetite suppression intensifies as the dose escalates. By the time you reach 1.0 mg (week 8), food noise is typically gone. A clinical study found semaglutide reduced ad libitum caloric intake by 38.9% versus placebo. Use the semaglutide dosage calculator to track your escalation schedule.
Can I lose weight on the 0.25 mg starting dose?
Yes, but the amount is modest. The 0.25 mg dose is a titration step designed to minimize GI side effects, not a therapeutic dose for weight loss. Most users lose 0.5-1% of body weight during the first 4 weeks at 0.25 mg. The significant weight loss begins at 0.5-1.0 mg and above. Do not stay at 0.25 mg longer than 4 weeks unless your prescriber specifically advises it. For the full dose schedule, see the semaglutide dosage chart in mL.
Why am I not losing weight on semaglutide after 2 weeks?
Two weeks is too early to evaluate weight loss results. The first 2 weeks are a tolerance-building phase at the lowest dose (0.25 mg). Real fat loss becomes measurable at weeks 3-4 and accelerates through months 2-3 as doses increase. If the scale has not moved after 6-8 weeks on escalating doses, check liquid calorie intake, injection technique, and product quality. Our full troubleshooting guide covers every scenario: not losing weight on semaglutide.
Does semaglutide work faster with exercise?
Exercise does not speed up when semaglutide starts working (appetite suppression begins in week 1 regardless), but it amplifies the total weight loss and improves body composition. A 2024 study found that combining semaglutide with supervised exercise preserved more lean muscle mass while increasing fat loss. Aim for 150 minutes of moderate activity per week plus 2-3 resistance training sessions. The combination also reduces the risk of semaglutide fatigue by maintaining metabolic rate.
How much weight can I lose in 3 months on semaglutide?
The STEP 1 clinical trial showed an average loss of 9.6% body weight at 12 weeks (3 months). For a 220 lb starting weight, that is approximately 21 lbs. For a 180 lb starting weight, approximately 17 lbs. Individual results range from 5% to 15% depending on dose tolerance, diet quality, exercise, and starting metabolic health. Users who pair semaglutide with a high-protein diet and regular exercise tend to hit the upper end. Compare your progress to real user data in our semaglutide before and after guide.
What happens if I stop taking semaglutide?
Weight regain is common after stopping. The STEP 1 trial extension found that participants regained two-thirds of lost weight within one year of discontinuation. Semaglutide stays in your system for approximately 5 weeks after the last injection, so its appetite-suppressing effects fade gradually rather than stopping abruptly. Most clinicians recommend continued treatment at a maintenance dose rather than full discontinuation. If cost is a concern, microdosing semaglutide at lower doses may sustain partial benefits.
Is semaglutide faster for weight loss than tirzepatide?
Both start suppressing appetite within the first week, so the initial onset speed is similar. Over time, tirzepatide produces more total weight loss: 22.5% at 72 weeks (SURMOUNT-1) versus 14.9% at 68 weeks (STEP 1) for semaglutide. Tirzepatide's dual GLP-1/GIP mechanism drives the additional loss. If semaglutide is not producing adequate results after 3-6 months, switching to tirzepatide is common. See our semaglutide to tirzepatide switching guide for the conversion protocol.
Do I need to change my diet on semaglutide?
Semaglutide reduces appetite automatically, so many users naturally eat less without formal dieting. However, what you eat still matters for speed of results and body composition. Prioritize protein (0.7-1.0 g per pound of target body weight) to preserve muscle mass. Minimize liquid calories (alcohol, sugary drinks, calorie-dense smoothies), which bypass semaglutide's satiety mechanism. Avoid large, fatty meals that worsen nausea. The best peptides for weight loss guide covers complementary strategies for maximizing results.
The Bottom Line
Semaglutide works faster than most users expect for appetite control and slower than most users hope for visible weight loss. The timeline is predictable: appetite changes in week 1, measurable scale movement by week 4, rapid loss through months 2-4, and a gradual plateau as you approach month 6-12. The STEP 1 trial confirmed an average of 14.9% body weight loss at 68 weeks, with 86.4% of participants losing at least 5%.
Your speed of results depends on four controllable factors: following the dose escalation schedule, eating adequate protein, exercising regularly, and eliminating liquid calories. Users who optimize all four consistently outperform the trial averages. Users who rely on the drug alone and change nothing else still lose weight, just less and slower.
Use the semaglutide dosage calculator to map your personal escalation timeline. If you are in the first month and wondering whether your experience is normal, it probably is. Give the drug 8 full weeks before judging results. If you are past 8 weeks with no progress, read not losing weight on semaglutide for a structured troubleshooting approach.
Not sure if semaglutide is the right peptide for your goals? Take our peptide quiz to get a personalized recommendation based on your health objectives, experience level, and preferences.
Related Articles: - Semaglutide Before and After - real user results with photos and timelines - Semaglutide Dosage Chart in mL - injection volumes for every dose level - Does Semaglutide Cause Nausea? - mechanism, incidence rates, and management - How Long Do Semaglutide Side Effects Last? - week-by-week resolution timeline - Not Losing Weight on Semaglutide - troubleshooting guide for stalls - Semaglutide to Tirzepatide Switching - conversion protocol when switching medications
Related Articles
How Long Does Semaglutide Take to Work?
Semaglutide reduces appetite within days, produces measurable weight loss at 4-8 weeks, and delivers significant results by 12-16 weeks.
Semaglutide Before and After Results
Semaglutide before and after results from STEP clinical trials: 5% weight loss at 2 months, 10% at 4 months, and 14.9% at 16 months.
Why Is My Semaglutide Red? Color Guide
Red or pink semaglutide means vitamin B12 was added by a compounding pharmacy. Brand Ozempic/Wegovy is always clear. Learn when color signals degradation.
How to Get Semaglutide: Prescription, Cost, Access
Get semaglutide via prescription, telehealth, or pharmacy. BMI eligibility, insurance coverage, brand vs. compounded costs, and step-by-step access guide for 2026.