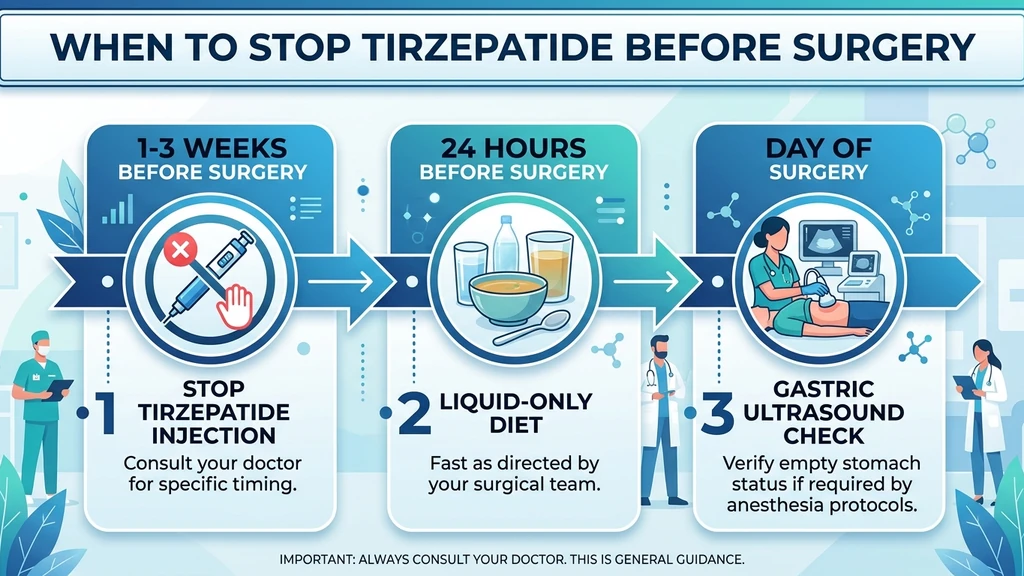
Your surgery date is set and you take tirzepatide weekly. The standard recommendation is to hold your last tirzepatide dose 1 to 3 weeks before surgery, depending on the procedure type and your individual risk factors. This timeline exists because tirzepatide slows gastric emptying by 30 to 40%, which can leave food in your stomach during anesthesia and raise the risk of pulmonary aspiration (ASA Consensus Guidance, 2023; Multi-Society Guidance, 2024).
| Guideline Source | Recommendation | Year |
|---|---|---|
| ASA Task Force | Hold weekly GLP-1 agonist 1 week before procedure | 2023 |
| Multi-Society (ASA/AGA/ASMBS/ISPCOP/SAGES) | Most patients can continue with risk stratification | 2024 |
| SPAQI Consensus | Hold 1 to 2 weeks; liquid diet 24 hours before | 2025 |
| ADS/ANZCA/GESA (Australia/NZ) | Routine cessation not recommended; manage per symptoms | 2025 |
The guidelines have evolved since 2023. Early guidance was conservative: stop all GLP-1 medications a full week before any procedure. The 2024 multi-society update took a more nuanced position, recognizing that blanket cessation is unnecessary for most patients. Your anesthesiologist's specific instructions should take priority over any general guidance. This article walks through the evidence, the risks, and how to navigate the decision with your surgical team.
For drug interaction concerns beyond surgery, see our full tirzepatide drug interactions guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Tirzepatide Creates Surgical Risk
Tirzepatide activates both GLP-1 and GIP receptors. The GLP-1 component slows the rate at which your stomach pushes food into the small intestine. In therapeutic terms, this delayed gastric emptying helps you feel full longer and lose weight. In surgical terms, it means your stomach may still contain food or liquid even after standard fasting.
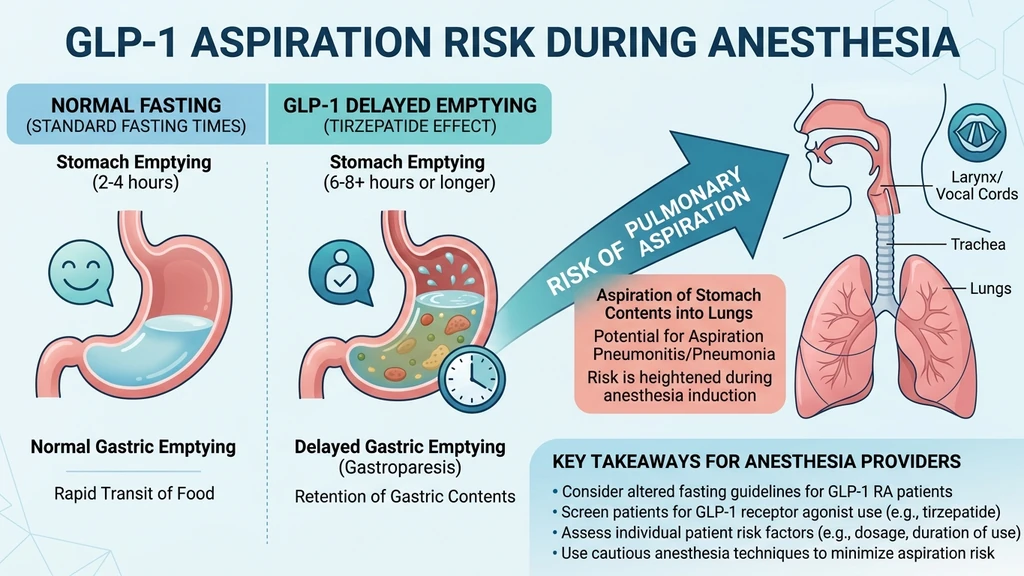
General anesthesia suppresses your cough reflex and relaxes the muscles that protect your airway. If your stomach holds residual food, that material can travel upward into the esophagus and enter the lungs. This event, called pulmonary aspiration, occurs in roughly 0.02 to 0.07% of elective surgeries in the general population. The concern with GLP-1 agonists is that delayed gastric emptying could push that rate higher (PMC, 2023).
Tirzepatide's Half-Life and Clearance Timeline
Tirzepatide has a half-life of approximately 5 days (120 hours). After your last injection, blood levels drop by half every 5 days. It takes roughly 4 to 5 half-lives (20 to 25 days) for the drug to clear your system almost entirely. For a detailed breakdown, see our guide on how long tirzepatide stays in your system.
| Days After Last Dose | Approximate Drug Remaining | Gastric Emptying Effect |
|---|---|---|
| 0 (injection day) | 100% | Maximum delay |
| 5 days | 50% | Significant delay |
| 10 days | 25% | Moderate delay |
| 15 days | 12.5% | Mild delay |
| 20 days | 6.25% | Minimal delay |
| 25 days | 3.1% | Near-normal |
This pharmacokinetic reality is why some conservative protocols recommend stopping 2 to 3 weeks before surgery rather than just one week. At one week, roughly 40 to 50% of the drug remains active. At two weeks, that drops to approximately 25%. The gastric emptying effect does not vanish the moment tirzepatide levels drop; it diminishes gradually.
Gastric Emptying Delay: What the Data Shows
The acetaminophen absorption test in tirzepatide's FDA prescribing information provides the clearest pharmacokinetic window into gastric emptying delay. After the first tirzepatide dose, acetaminophen peak concentration (Cmax) dropped 50 to 55%, and the time to peak (Tmax) shifted from 0.5 hours to 2.5 hours. Total absorption (AUC) fell only 15 to 20% (FDA Prescribing Information, 2025).
At steady state on 5 mg, the delay partially normalizes through tachyphylaxis. Patients who have been on a stable dose for 4 or more weeks experience less gastric emptying delay than those in the dose-escalation phase. This is why the 2024 multi-society guidance differentiates between patients in escalation versus maintenance.
A 2024 study using gastric scintigraphy found that 56% of GLP-1 receptor agonist users had significant gastric retention after standard fasting, compared to 19% in controls (PMC, 2024). The clinical meaning: standard fasting protocols (nothing by mouth after midnight) may not empty the stomach of a tirzepatide user as reliably as they do for someone not on the medication.
Current Medical Guidelines: ASA, AGA, and Multi-Society Recommendations
Guidelines have shifted significantly between 2023 and 2025. Understanding the evolution helps you interpret what your surgical team recommends and ask informed questions.
ASA 2023 Consensus Guidance (Original)
The American Society of Anesthesiologists released its first GLP-1 perioperative guidance in June 2023. The recommendation was straightforward: hold GLP-1 receptor agonists on the day of or the week before elective procedures (ASA, 2023).
For weekly formulations like tirzepatide, this meant skipping your last scheduled dose before surgery. If your injection was due on Monday and surgery was Friday, you would skip that Monday dose. The guidance acknowledged limited evidence and leaned toward caution.
The 2023 guidance also introduced a key practical measure: if surgery cannot be delayed and the patient has GI symptoms (nausea, vomiting, bloating, abdominal pain), treat as a "full stomach" case. This means rapid-sequence intubation with cricoid pressure to protect the airway during anesthesia induction.
2024 Multi-Society Clinical Practice Guidance (Updated)
In October 2024, five major medical societies (ASA, AGA, ASMBS, ISPCOP, and SAGES) published a joint guidance document that significantly revised the approach. The core message: most patients can continue GLP-1 receptor agonists before elective surgery with appropriate risk stratification (Multi-Society Guidance, 2024; AGA Summary, 2024).
The updated guidance identifies risk factors that elevate aspiration concern:
- Dose-escalation phase (first 4 to 8 weeks at any dose level)
- Active GI symptoms (nausea, vomiting, bloating, constipation, diarrhea)
- Higher doses (10 mg and 15 mg tirzepatide carry more GI effect than 2.5 mg and 5 mg)
- Weekly formulations (more GI symptoms than daily alternatives)
- History of gastroparesis or diabetic autonomic neuropathy
For patients without these risk factors who have been on a stable maintenance dose with no GI symptoms, the guidance allows continuation with a 24-hour liquid diet and point-of-care gastric ultrasound before the procedure.
For patients with risk factors, the guidance recommends holding tirzepatide for 1 to 2 weeks and following a liquid diet for at least 24 hours before surgery. If retained gastric contents are found on ultrasound, shared decision-making between the patient and anesthesiologist determines whether to proceed with full-stomach precautions or cancel.
SPAQI 2025 Consensus Statement
The Society for Perioperative Assessment and Quality Improvement published a multidisciplinary consensus in 2025 that added granularity to the hold period. Their recommendation: hold weekly GLP-1 agonists for 1 to 2 weeks before elective surgery, with the specific duration based on dose, GI symptom burden, and procedure type (SPAQI, 2025).
SPAQI emphasized point-of-care gastric ultrasound as a decision-making tool on the day of surgery. If the antral cross-sectional area suggests gastric volume below 1.5 mL/kg, proceed normally. If above that threshold, consider postponement or rapid-sequence intubation.
2025 Australian/New Zealand Recommendations
The ADS/ANZCA/GESA/NACOS joint recommendations, published in 2025, took the most permissive stance. They concluded that elective preprocedural cessation of GLP-1 and GLP-1/GIP receptor agonists is not recommended (ADS/ANZCA/GESA, 2025).
Their rationale: omitting a long-acting GLP-1 agonist for 1 to 2 weeks is unlikely to meaningfully alter the GLP-1-induced slowing of gastric emptying, given the drug's prolonged half-life. Instead, they recommend enhanced fasting protocols (clear liquids only for 24 hours) and point-of-care gastric ultrasound for all GLP-1 patients, regardless of whether the medication was held.
This position reflects a growing view that the gastric emptying effect persists beyond the drug's active window, making short-term cessation less effective than previously assumed.
Timing by Surgery Type: Specific Recommendations
Not all surgeries carry equal aspiration risk. The type of anesthesia, the position of your body during the procedure, and the urgency of the surgery all determine how aggressively your team should manage tirzepatide timing.
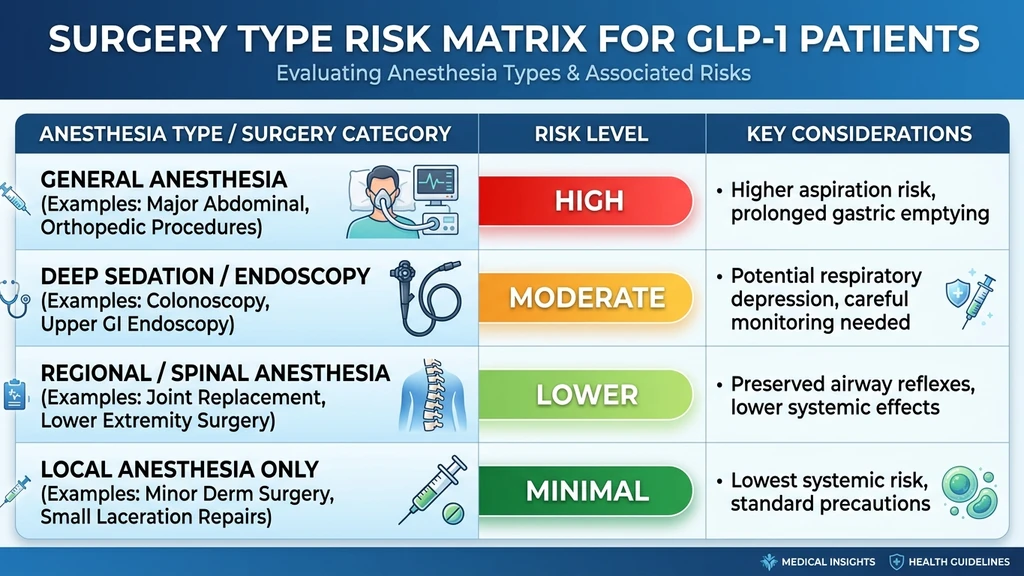
General Anesthesia (Highest Risk)
General anesthesia involves intubation (placing a breathing tube through your mouth into your trachea). During the induction phase, when you transition from awake to unconscious, your protective airway reflexes are absent. This is the window where aspiration occurs.
Recommended hold period: 1 to 3 weeks before surgery.
The conservative end (3 weeks) applies to patients on high doses (10 to 15 mg), those in dose escalation, or those with active GI symptoms. The moderate end (1 to 2 weeks) applies to stable maintenance-dose patients without GI complaints. If your surgeon's office gives you a specific timeline, follow it.
Procedures under general anesthesia include: abdominal surgery, joint replacement, cardiac surgery, most orthopedic procedures, and any operation lasting more than 2 hours. For patients considering body contouring surgery after tirzepatide weight loss, this timeline is particularly relevant because these procedures are elective and can be scheduled around the hold period.
Deep Sedation and Endoscopy (Moderate Risk)
Deep sedation (propofol-based) suppresses airway reflexes similarly to general anesthesia, though the duration is shorter. Upper endoscopy (EGD) carries additional risk because the scope passes through the esophagus, potentially stimulating regurgitation.
Recommended hold period: 1 to 2 weeks, or follow AGA rapid practice update.
The AGA published a rapid clinical practice update in 2023 specifically addressing GLP-1 patients before endoscopy. They recommend considering holding GLP-1 agonists for at least one dosing interval before upper endoscopy. For tirzepatide, that means skipping one weekly dose (AGA, 2023).
A 24-hour liquid diet before endoscopy reduces residual gastric contents. If food is found during the procedure, the endoscopist can suction it, but this increases procedure time and complication risk. Colonoscopy (lower endoscopy) carries minimal aspiration risk because the scope does not involve the upper GI tract, and the bowel prep itself clears the system.
Regional and Spinal Anesthesia (Lower Risk)
Regional anesthesia (nerve blocks, epidurals, spinal blocks) does not suppress airway reflexes because you remain conscious or lightly sedated. The aspiration risk is substantially lower than general anesthesia.
Recommended hold period: Consider holding 1 week, but continuation may be acceptable.
Procedures commonly performed under regional anesthesia include: cesarean delivery, knee arthroscopy, hand and wrist surgery, and many orthopedic procedures below the waist. Your anesthesiologist may still recommend holding tirzepatide as a precaution, especially if there is any chance the regional block could fail and general anesthesia would be needed as a backup.
For joint injections, minor nerve blocks, or epidural steroid injections, tirzepatide continuation is generally acceptable. These procedures use local anesthetic and do not involve airway management.
Local Anesthesia Only (Minimal Risk)
Procedures performed entirely under local anesthesia (dental work, skin biopsies, minor wound repairs, trigger point injections) carry no aspiration risk because airway reflexes remain fully intact. No sedation is involved.
Tirzepatide does not need to be stopped for local-only procedures.
However, verify with your provider that no sedation is planned. "Local with sedation" is a common combination for procedures like wisdom tooth extraction or breast biopsies, and the sedation component reintroduces some airway risk. If IV sedation is part of the plan, treat the procedure as moderate risk.
Emergency Surgery
Emergency surgery does not allow time for a planned medication hold. If you arrive at the emergency department on tirzepatide, your anesthesiologist will use "full stomach precautions" regardless of your last dose timing.
Full stomach protocol includes: rapid-sequence intubation (RSI), cricoid pressure during induction, head-of-bed elevation to 30 degrees, and possibly gastric decompression with a nasogastric tube before induction. These measures are routine for emergency surgery in all patients, not just those on GLP-1 medications.
Inform the surgical team that you take tirzepatide (Mounjaro or Zepbound), the dose, and when your last injection was. This information helps the anesthesiologist plan. Carry this information in your wallet or phone medical ID. Review our peptide safety guide for additional preparedness recommendations.
The Pre-Surgery Checklist: Step-by-Step Protocol
Use this timeline to prepare for elective surgery while on tirzepatide. Adjust the hold period based on your anesthesiologist's specific instructions.
3 to 4 Weeks Before Surgery
Schedule a pre-operative appointment with your surgeon and anesthesiologist. Bring a complete medication list that includes tirzepatide, the brand name (Mounjaro or Zepbound), your current dose, and the day of the week you inject. For dose reference, use our tirzepatide dosage calculator.
Discuss the hold plan. Ask: "Should I skip my last dose, my last two doses, or continue with modifications?" The answer depends on your dose level, GI symptom history, and the type of anesthesia planned.
If you are in the dose-escalation phase, your team may recommend a longer hold period. If you are on a stable maintenance dose with no GI symptoms, the hold may be shorter or unnecessary with enhanced fasting protocols.
1 to 3 Weeks Before Surgery (Medication Hold)
Stop tirzepatide on the date your surgical team specifies. Do not take an extra dose to "stock up" before the hold period. Tirzepatide's long half-life means the drug continues working for days after your last injection.
During the hold period, you may notice: - Increased appetite (GLP-1 satiety effect fading) - Mild blood sugar fluctuations if you have type 2 diabetes - No significant weight regain in 1 to 3 weeks
If you have type 2 diabetes, discuss blood sugar management during the hold period with your endocrinologist. You may need temporary insulin adjustments. Check our guide on tirzepatide drug interactions for any other medications that may need adjustment.
24 to 48 Hours Before Surgery
Switch to a liquid-only diet for 24 hours (or 48 hours if your team requests it). Clear liquids include: water, broth, clear juice without pulp, gelatin, and black coffee or tea. Avoid milk, smoothies, protein shakes, and anything opaque.
The liquid diet compensates for any residual gastric emptying delay. Even patients who held tirzepatide for 2 weeks benefit from this step because the gastric emptying effect may persist beyond the drug's measured half-life.
Follow standard NPO (nil per os) timing for the day of surgery. Most institutions require: no solid food for 8 hours before anesthesia, clear liquids permitted up to 2 hours before. Your surgical center may have stricter rules for GLP-1 patients.
Day of Surgery
Your anesthesiologist may perform a point-of-care gastric ultrasound before induction. This bedside test takes 2 to 3 minutes and shows whether your stomach contains solid food, liquid, or is empty. The antral cross-sectional area measurement correlates with gastric volume.
If the ultrasound shows an empty or near-empty stomach (less than 1.5 mL/kg estimated volume), surgery proceeds normally. If significant gastric contents are found, three options exist:
- 1.Proceed with rapid-sequence intubation (RSI): Faster induction with airway protection. Standard for full-stomach cases.
- 2.Delay the procedure: Wait 2 to 4 hours and recheck. Gastric contents may clear with additional fasting.
- 3.Cancel and reschedule: If the risk-benefit calculation favors postponement, especially for purely elective procedures.
Shared decision-making between you and the anesthesiologist determines the path. For urgent procedures, option 1 is typical. For elective cosmetic or non-urgent orthopedic surgery, option 3 may be safest.
Aspiration Risk: Understanding the Real Danger
Pulmonary aspiration during anesthesia is rare but potentially fatal. Stomach contents entering the lungs cause chemical pneumonitis (acid burns to lung tissue), bacterial pneumonia, acute respiratory distress syndrome (ARDS), or airway obstruction. Mortality rates for severe aspiration events range from 5 to 30%, depending on the volume and acidity of the aspirated material (PMC, 2023).
How Common Is Aspiration in GLP-1 Patients?
The background aspiration rate during elective surgery is 0.02 to 0.07% (2 to 7 per 10,000 cases). The critical question is whether GLP-1 agonists meaningfully increase this rate. Current data is mixed.
A 2023 case series reported several cases of retained gastric contents and aspiration events in patients taking semaglutide or tirzepatide who had followed standard fasting guidelines (PMC, 2023). These cases prompted the ASA's initial 2023 guidance.
However, larger retrospective analyses have not consistently shown a statistically significant increase in aspiration rates among GLP-1 users. A 2024 analysis cited in the multi-society guidance suggested the absolute risk increase, if any, is small. The challenge: GLP-1 agonist use has expanded so rapidly that large-scale prospective data does not yet exist.
The practical takeaway: the risk is real but uncommon. The precautions (medication hold, liquid diet, gastric ultrasound) are proportionate responses that reduce an already-low risk to near baseline. Skipping these precautions is not worth the gamble. For more on GI side effects that may compound this risk, see our article on whether semaglutide causes nausea.
Risk Factors That Increase Aspiration Danger
Not every tirzepatide patient carries the same aspiration risk. The multi-society guidance identifies factors that move you from standard risk to elevated risk:
Higher risk: - Dose-escalation phase (first 4 weeks at each new dose) - Active nausea, vomiting, or bloating - Higher doses (10 mg or 15 mg tirzepatide) - History of gastroparesis or slow gastric emptying - Diabetes with autonomic neuropathy - Concurrent opioid use (opioids independently slow gastric emptying) - Obesity (higher baseline aspiration risk)
Lower risk: - Stable maintenance dose for 4 or more weeks - No GI symptoms - Lower doses (2.5 mg or 5 mg tirzepatide) - No history of gastroparesis - No concurrent opioid use
If you fall entirely in the lower-risk category, your anesthesiologist may allow tirzepatide continuation with enhanced fasting protocols. If you have multiple higher-risk factors, a 2 to 3 week hold is prudent.
Anesthesia Modifications for GLP-1 Patients
When your anesthesiologist knows you take tirzepatide, several modifications to the standard anesthesia plan become available. These reduce aspiration risk even if the medication was not held or was held for a shorter period.
Rapid-Sequence Intubation (RSI)
RSI is the primary airway protection technique for patients at aspiration risk. Instead of the standard slow induction (preoxygenation, induction agent, waiting for muscle relaxation, gentle mask ventilation, then intubation), RSI compresses the timeline.
The sequence: preoxygenation, induction agent and fast-acting paralytic (succinylcholine or high-dose rocuronium) administered simultaneously, cricoid pressure applied to compress the esophagus and prevent regurgitation, and immediate intubation without mask ventilation. The entire sequence takes 60 to 90 seconds.
RSI is a well-established technique used thousands of times daily for emergency surgery, pregnant patients, and anyone with suspected full stomach. It is not a drastic measure. If your anesthesiologist recommends RSI because of your tirzepatide use, this is standard risk mitigation.
Point-of-Care Gastric Ultrasound
Gastric ultrasound has become the key decision-making tool for GLP-1 patients. Using a standard curvilinear ultrasound probe placed over the epigastric area, the anesthesiologist can visualize the gastric antrum and estimate stomach contents in real time.
The classification system: - Grade 0 (empty): Antrum appears flat or empty in both supine and right lateral positions. Proceed normally. - Grade 1 (clear liquid): Small amount of clear fluid visible. Low risk. Proceed in most cases. - Grade 2 (solid or thick liquid): Solid content or turbid fluid visible. Elevated aspiration risk. Consider RSI or delay.
The antral cross-sectional area (CSA) can be measured and converted to an estimated gastric volume using validated formulas. A volume below 1.5 mL/kg is generally considered safe. Above that threshold, the team discusses whether to proceed with RSI, delay, or cancel.
This tool has changed the conversation from "hold the medication for everyone" to "assess the individual patient on the day of surgery." It explains why the newer guidelines are more permissive than the original 2023 ASA guidance.
Enhanced Fasting Protocols
Standard NPO guidelines (8 hours for solids, 2 hours for clear liquids) were designed for the general population. For tirzepatide patients, enhanced fasting adds a margin of safety.
Enhanced protocols typically include: - Clear liquid diet for 24 hours before surgery (not just overnight) - Nothing by mouth for 8 to 12 hours (extended from the standard 6 to 8 hours for solids) - Avoidance of high-fat and high-fiber meals for 48 hours before surgery - No alcohol for 48 hours (alcohol independently delays gastric emptying; see our guide on alcohol and tirzepatide)
Some institutions add prokinetic agents (metoclopramide 10 mg orally the night before and morning of surgery) to accelerate gastric emptying. Prokinetics are not universally recommended but are an option for higher-risk patients.
Restarting Tirzepatide After Surgery
The restart timeline depends on the type of surgery, your recovery, and your GI function. Restarting too early can worsen postoperative nausea and vomiting (PONV) and slow your recovery. Restarting too late means unnecessary time off medication.
General Timeline for Resumption
Most surgical teams recommend restarting tirzepatide once you meet all of the following criteria:
- 1.Tolerating a regular diet (not just liquids or soft foods)
- 2.No active nausea or vomiting for at least 24 hours
- 3.Bowel function has returned (passing gas or having a bowel movement)
- 4.Surgeon clearance given at the postoperative visit
For minor outpatient procedures (endoscopy, dental surgery under sedation, small skin excisions), this may be as soon as 24 to 48 hours after the procedure. For major abdominal surgery, it may take 1 to 2 weeks or longer.
| Surgery Type | Typical Restart Timeline |
|---|---|
| Endoscopy/colonoscopy | 24 to 48 hours |
| Minor outpatient (dental, skin) | 24 to 48 hours |
| Orthopedic (joint replacement) | 3 to 7 days |
| Abdominal surgery | 1 to 2 weeks (once eating normally) |
| Bariatric surgery | Per bariatric surgeon (often 2 to 4 weeks) |
| Cardiac surgery | Per cardiologist (often 1 to 2 weeks) |
Restarting at the Same Dose vs. Dose Reduction
If you held tirzepatide for 1 to 2 weeks, you can typically restart at your previous dose. The drug's long half-life means some active tirzepatide remains in your system, reducing the re-initiation effect.
If you held tirzepatide for 3 weeks or longer, discuss with your prescriber whether to restart at a lower dose and re-escalate. The tachyphylaxis (tolerance) that developed during your original escalation has partially reversed during the hold. Restarting at your full dose after a prolonged break may produce stronger GI side effects (nausea, vomiting, diarrhea) than you experienced at that dose previously.
A reasonable approach for a 3-plus-week hold: restart one dose level below your maintenance dose for 2 weeks, then return to maintenance. For example, if you were on 10 mg, restart at 7.5 mg for two weeks, then resume 10 mg. For detailed dose charts, see our tirzepatide dosage chart or compound tirzepatide dosage chart.
Managing Blood Sugar During the Hold Period
Patients with type 2 diabetes face an additional challenge: tirzepatide provides substantial blood glucose control, and holding it before surgery means losing that glycemic effect. Perioperative hyperglycemia (blood sugar above 180 mg/dL) increases surgical site infection rates, delays wound healing, and worsens outcomes.
Work with your endocrinologist to create a bridging plan. Options include:
- Temporary basal insulin (glargine or detemir) to cover the gap
- Increased metformin dose (if not already at maximum and renal function is adequate)
- Frequent blood glucose monitoring (4 times daily during the hold period)
- Sliding-scale insulin for day-of-surgery glucose management
Do not attempt to manage this transition alone. Diabetes medication changes require medical supervision, especially around surgery. Your endocrinologist and surgical team should coordinate the plan.
Special Populations and Considerations
Certain patient groups require additional attention when planning tirzepatide cessation around surgery.
Patients with Gastroparesis
Gastroparesis (delayed gastric emptying without mechanical obstruction) affects 2 to 4% of the general population and is more common in patients with diabetes. Tirzepatide adds pharmaceutical gastric emptying delay on top of an already-slow baseline.
For patients with known gastroparesis, the hold period should be at the conservative end: 2 to 3 weeks before surgery. Enhanced fasting (48-hour liquid diet) and gastric ultrasound on the day of surgery are strongly recommended. Some anesthesiologists will require a normal gastric ultrasound before proceeding, regardless of how long the medication was held.
If you have gastroparesis and take tirzepatide, always inform your anesthesiologist of both conditions. They compound each other's risk.
Patients on Concurrent Opioids
Opioids independently slow gastric emptying. Patients taking chronic opioid therapy (for pain management) alongside tirzepatide face additive gastric emptying delay. This combination places you in the higher-risk category regardless of your tirzepatide dose or symptom burden.
A longer hold period (2 to 3 weeks) and enhanced fasting protocols are advisable. Point-of-care gastric ultrasound is essential before proceeding. If your opioid is prescribed for chronic pain and the surgery is expected to require postoperative opioids, the combined effect on gastric motility during recovery also affects the restart timeline.
Pregnant or Planning Pregnancy
Tirzepatide is contraindicated in pregnancy. If you discover you are pregnant before scheduled surgery, tirzepatide should be discontinued immediately regardless of the surgical timeline. The FDA recommends stopping tirzepatide at least 2 months before a planned pregnancy due to the drug's long washout period.
For pregnant patients requiring emergency surgery, the anesthesiologist already uses full-stomach precautions (RSI) as standard practice because pregnancy itself delays gastric emptying and increases aspiration risk. Prior tirzepatide use does not change the emergency anesthesia protocol but should be disclosed to the team. See our tirzepatide long-term side effects guide for additional reproductive safety information.
Switching Between GLP-1 Medications Before Surgery
Some patients consider switching from tirzepatide to a shorter-acting GLP-1 agonist (like daily liraglutide) before surgery, reasoning that a daily formulation would clear faster after the last dose. This approach is not recommended by any guideline.
Switching GLP-1 medications introduces a new escalation phase with unpredictable GI side effects. The GLP-1-mediated gastric emptying delay is a class effect, not unique to tirzepatide. Liraglutide causes similar gastric emptying delay despite its shorter half-life. The net result of switching: new GI symptoms, uncertain gastric emptying patterns, and no clear safety advantage.
If you are considering switching from semaglutide to tirzepatide or vice versa for reasons unrelated to surgery, see our semaglutide-to-tirzepatide switching guide and time the transition to avoid proximity to any planned procedures.
What to Tell Your Surgical Team
Clear communication with your surgical team is the most important factor in safe perioperative management. Provide the following information at your pre-operative visit and again on the day of surgery.
Information Your Anesthesiologist Needs
Prepare a brief summary:
- Medication name: Tirzepatide (Mounjaro for type 2 diabetes, Zepbound for weight management)
- Current dose: (2.5 mg, 5 mg, 7.5 mg, 10 mg, or 15 mg)
- Injection day: Which day of the week you normally inject
- Date of last injection: The exact date of your most recent dose
- GI symptoms: Whether you currently experience nausea, vomiting, bloating, or constipation
- Phase: Whether you are in dose escalation or on a stable maintenance dose
- Diabetes status: Whether you take tirzepatide for type 2 diabetes or weight management only
- Other GLP-1 history: Whether you previously took semaglutide or another GLP-1 agonist
This information allows the anesthesiologist to risk-stratify you accurately and choose the appropriate management approach. Do not assume the surgical team knows you take tirzepatide. Many patients fail to mention injectable medications during pre-operative interviews. For injection technique and administration details you might need after resumption, keep our guide bookmarked.
Questions to Ask Your Surgeon and Anesthesiologist
Arrive at your pre-operative visit with specific questions:
- 1."How many weeks before surgery should I hold my tirzepatide?"
- 2."Should I follow a liquid diet before surgery, and for how long?"
- 3."Will you perform a gastric ultrasound on the day of surgery?"
- 4."If the ultrasound shows food in my stomach, will you proceed or reschedule?"
- 5."When can I restart tirzepatide after surgery?"
- 6."Should I restart at my full dose or a lower dose?"
- 7."Do I need insulin coverage during the hold period?" (if diabetic)
These questions demonstrate informed engagement and help your team create a personalized plan. The answers vary by institution, surgeon preference, and your individual risk profile.
Tirzepatide vs. Semaglutide: Does Surgery Timing Differ?
Both tirzepatide and semaglutide are weekly GLP-1 receptor agonists, and both delay gastric emptying. The perioperative guidelines apply to both medications equally. However, there are pharmacological differences worth noting.
Pharmacokinetic Comparison
Tirzepatide's half-life is approximately 5 days. Semaglutide's half-life is approximately 7 days (168 hours). This means semaglutide lingers longer after the last dose.
| Parameter | Tirzepatide | Semaglutide |
|---|---|---|
| Half-life | ~5 days | ~7 days |
| Time to near-complete clearance | 20 to 25 days | 28 to 35 days |
| Mechanism | GLP-1 + GIP dual agonist | GLP-1 single agonist |
| Gastric emptying delay | 30 to 40% | 25 to 35% |
| Recommended hold period | 1 to 3 weeks | 1 to 4 weeks |
In practice, most anesthesiologists apply the same hold period for both medications. The extra GIP receptor activity in tirzepatide does not appear to add independent gastric emptying risk beyond the GLP-1 effect. If you are switching between these medications, allow at least 2 weeks between the last semaglutide dose and the first tirzepatide dose (or vice versa), and do not schedule surgery during the transition.
Daily vs. Weekly Formulations
Daily GLP-1 agonists (liraglutide/Saxenda, oral semaglutide/Rybelsus) have shorter half-lives. Liraglutide's half-life is 13 hours, meaning it clears the body in 2 to 3 days after the last dose. Oral semaglutide has a half-life of approximately 7 days despite daily dosing because of its albumin binding.
For daily liraglutide, the hold period is shorter: the ASA originally recommended holding on the day of surgery. The 2024 multi-society guidance suggests holding daily formulations for 1 day before surgery with the same risk-stratification approach.
The bottom line: weekly tirzepatide requires a longer pre-surgical hold than daily liraglutide, but the same duration as weekly semaglutide. The guidelines do not differentiate between Mounjaro and Zepbound (both are tirzepatide) or between Ozempic and Wegovy (both are semaglutide). Brand name does not change the pharmacology.
Common Mistakes to Avoid
Patients and even some healthcare providers make predictable errors when managing tirzepatide around surgery. Avoiding these mistakes reduces your risk.
Mistake 1: Not Disclosing Tirzepatide Use
The most dangerous error. If your anesthesiologist does not know you take tirzepatide, they will use standard induction protocols that assume a normal, empty stomach after standard fasting. Survey data suggests 20 to 30% of patients fail to report injectable medications during pre-operative assessments.
Tirzepatide is not listed on many hospital formularies because it is typically prescribed by outpatient providers. The medication may not appear in your hospital medical record. You must proactively disclose it. Consider wearing a medical alert bracelet or adding tirzepatide to your phone's medical ID (accessible from the lock screen on most smartphones).
Mistake 2: Stopping Too Early and Losing Glycemic Control
Overly conservative patients sometimes stop tirzepatide 4 to 6 weeks before surgery. While this ensures complete drug clearance, it sacrifices weeks of blood sugar control. For type 2 diabetes patients, this can lead to perioperative hyperglycemia, which directly worsens surgical outcomes.
The evidence does not support holds longer than 3 weeks. Even the most conservative guidelines recommend 2 to 3 weeks maximum. Longer holds require insulin bridging, add complexity, and offer no proven additional safety benefit. For context on tirzepatide's shelf life and stability during the hold period, unused pens can be stored according to standard guidelines.
Mistake 3: Ignoring the Liquid Diet Recommendation
Some patients hold tirzepatide for the recommended period but then eat a normal meal the night before surgery. The liquid diet is not optional decoration on the protocol. Residual gastric emptying delay can persist beyond the drug's measured half-life, and a heavy meal the night before surgery may not fully clear by morning.
Clear liquids for 24 hours before surgery is the minimum. If your team recommends 48 hours of liquids, follow the instruction. For guidance on food choices during the pre-operative period, our guide on what to eat on tirzepatide covers tolerable options.
Mistake 4: Restarting Tirzepatide Too Soon After Surgery
Postoperative nausea and vomiting (PONV) affects 30 to 40% of surgical patients. Restarting tirzepatide while you still have PONV amplifies the nausea. General anesthesia itself slows gastric motility for 24 to 48 hours. Adding tirzepatide's GLP-1 effect on top of post-anesthetic gastroparesis creates a compounding problem.
Wait until you are eating solid food comfortably, with no nausea, before restarting. Rushing the restart to avoid weight regain is understandable but counterproductive if it triggers vomiting that delays your surgical recovery.
Frequently Asked Questions
How many weeks before surgery should I stop tirzepatide?
The standard recommendation is 1 to 3 weeks before surgery. The 2023 ASA guidance recommended holding weekly GLP-1 agonists for 1 week. The 2024 multi-society update allows continuation for low-risk patients with enhanced fasting protocols. Conservative practice holds tirzepatide for 2 to 3 weeks for major surgery under general anesthesia. Follow your specific anesthesiologist's instructions, which should be based on your dose, symptoms, and procedure type. Use our tirzepatide dosage calculator to verify your current dose level.
Can I take Mounjaro the week of surgery?
It depends on your risk profile. If you are on a stable maintenance dose with no GI symptoms and your surgery uses regional or local anesthesia, your team may permit continuation with a 24-hour liquid diet. For general anesthesia procedures, most anesthesiologists prefer you skip at least one weekly dose. The 2024 multi-society guidance does not mandate cessation for all patients but recommends risk stratification. Discuss your specific situation with your surgical team and review our tirzepatide drug interactions guide for additional medication considerations.
What happens if I don't stop tirzepatide before surgery?
If you did not hold tirzepatide and this is discovered on the day of surgery, your anesthesiologist has three options: proceed with rapid-sequence intubation (full-stomach precautions), delay the procedure by several hours and recheck your stomach with ultrasound, or cancel and reschedule. For emergency surgery, the team will always proceed with full-stomach precautions. The risk of not stopping is retained gastric contents that could be aspirated into your lungs during anesthesia. This risk is manageable with RSI but avoidable with planning. Read our peptide safety guide for broader safety protocols.
Does tirzepatide need to be stopped before a colonoscopy?
Colonoscopy (lower endoscopy) carries minimal aspiration risk because the scope does not enter the upper GI tract, and the bowel prep itself clears your system thoroughly. However, if your colonoscopy is performed under deep sedation or combined with an upper endoscopy (EGD), the aspiration risk increases. The AGA recommends holding GLP-1 agonists for at least one dosing interval before upper endoscopy. For a colonoscopy-only procedure under moderate sedation, tirzepatide continuation with a standard bowel prep is generally acceptable. Confirm with your gastroenterologist. Learn more about how tirzepatide affects your GI system in our guide on how long tirzepatide stays in your system.
When can I restart tirzepatide after surgery?
Restart once you tolerate a regular solid diet without nausea or vomiting and your surgeon gives clearance. For minor procedures, this is typically 24 to 48 hours. For major surgery, expect 1 to 2 weeks. If you held tirzepatide for less than 3 weeks, restart at your previous dose. If the hold exceeded 3 weeks, consider restarting one dose level lower for 2 weeks to minimize GI side effects. For post-surgical dose planning, see our tirzepatide maintenance dose guide.
Do I need to stop Zepbound before dental surgery?
It depends on the type of anesthesia. Dental procedures under local anesthesia only (numbing injections, no sedation) do not require stopping Zepbound. If your dental surgery involves IV sedation or general anesthesia (common for wisdom tooth extraction, dental implants, or complex oral surgery), treat it as a moderate-risk procedure and hold tirzepatide for at least 1 week. Follow a liquid diet for 24 hours before the procedure. Verify the anesthesia plan with your oral surgeon before your appointment. For injection-related questions after resumption, see our how to inject tirzepatide guide.
Will I gain weight if I stop tirzepatide for surgery?
Significant weight regain in 1 to 3 weeks is unlikely. Tirzepatide's half-life is approximately 5 days, so the appetite-suppressing effect fades gradually over 2 to 3 weeks rather than disappearing immediately. You may notice increased hunger during the second and third weeks of the hold. Focus on maintaining your eating patterns and portion sizes during this period. Any minor weight fluctuation from the hold is quickly reversed once you restart. For strategies to maintain weight loss long-term, see our tirzepatide before and after results guide.
Is gastric ultrasound required before surgery for tirzepatide patients?
Gastric ultrasound is recommended but not universally required. The 2024 multi-society guidance and SPAQI 2025 consensus both endorse point-of-care gastric ultrasound as a decision-making tool for GLP-1 patients. Not all institutions have ultrasound-trained anesthesiologists or equipment available in every operating room. If your facility does not offer gastric ultrasound, your anesthesiologist will rely on clinical assessment (symptom history, fasting duration, medication hold period) to determine the safest approach. Ask during your pre-operative visit whether gastric ultrasound will be available. For understanding how tirzepatide affects gastric emptying, review our drug interactions guide.
The Bottom Line
Stopping tirzepatide before surgery requires balancing aspiration risk against the benefits of continued treatment. The 2024 multi-society guidance moved the field away from blanket cessation toward individualized risk stratification. For most patients on a stable maintenance dose without GI symptoms, the hold period is 1 to 2 weeks combined with a 24-hour liquid diet and point-of-care gastric ultrasound. For patients in dose escalation, on high doses, or with active GI symptoms, 2 to 3 weeks is the safer choice.
The single most important action is communicating with your surgical team. Disclose your tirzepatide use, your current dose, your last injection date, and any GI symptoms. This information lets your anesthesiologist choose the right strategy: standard induction, rapid-sequence intubation, or enhanced fasting with gastric ultrasound.
Restarting after surgery follows a simple rule: wait until you eat solid food comfortably without nausea. For holds under 3 weeks, resume your previous dose. For longer holds, step down one dose level for 2 weeks before returning to maintenance.
Plan your tirzepatide dosing around your surgical schedule. Review your full medication list with our peptide interaction checker before the pre-operative visit. For broader safety protocols across all peptide use, bookmark our peptide safety guide.
Helpful Tools
Related Articles
Does Tirzepatide Help With Inflammation?
Does tirzepatide help with inflammation? Yes: CRP drops 32.9%, IL-6 drops 17.8% in trials. SURMOUNT data and adipose tissue mechanisms.
Does Compounded Tirzepatide Work? Real Data
Does compounded tirzepatide work? Review SURMOUNT data, salt form differences (base, acetate, sodium), potency gaps, and FDA status in 2026.
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
Does Tirzepatide Affect Your Period?
Does tirzepatide affect your period? Yes, via rapid fat loss and estrogen shifts. Cycle changes, PCOS fertility, and birth control warning.