
You stare at the prefilled pen on your bathroom counter and wonder if there is a world where this weekly ritual becomes swallowing a tablet with breakfast instead. Tirzepatide does not come in pill form as of March 2026. It is available only as a subcutaneous injection under the brand names Mounjaro (type 2 diabetes) and Zepbound (obesity). Eli Lilly is developing oral GLP-1 alternatives, but none contain tirzepatide itself.
| Quick Reference | Details |
|---|---|
| Tirzepatide pill available? | No. Injection only (March 2026) |
| Brand names | Mounjaro (diabetes), Zepbound (obesity) |
| Injection frequency | Once weekly, subcutaneous |
| Oral GLP-1 on market | Oral semaglutide (Rybelsus), 14 mg daily |
| Lilly oral pipeline | Orforglipron (oral GLP-1 agonist, Phase 3) |
| Oral tirzepatide timeline | No announced clinical program |
| Key barrier | Peptide degradation in stomach acid |
| Evidence level | FDA labels, ClinicalTrials.gov registrations |
The distinction matters because patients who fear needles often delay treatment, losing months of potential weight loss. Understanding what is available now, what is coming, and why oral peptides are so difficult to formulate helps you make an informed decision about starting injectable tirzepatide today rather than waiting for a pill that may be years away. For dosing protocols, see our tirzepatide dosage chart. For safety information, see our peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Tirzepatide Is Injection-Only Right Now
Tirzepatide is a 39-amino-acid peptide with a molecular weight of approximately 4,810 daltons. That number tells you almost everything about why it cannot be swallowed in a tablet. Peptides above roughly 1,000 daltons face severe absorption barriers in the gastrointestinal tract. The stomach produces hydrochloric acid at pH 1.5-3.5 and pepsin, a protease enzyme whose sole purpose is dismantling peptide bonds. Tirzepatide would be digested before reaching the small intestine. For a full breakdown of why swallowed versions fail and what actually works, see does oral tirzepatide work.
Think of it like mailing a letter made of sugar through a rainstorm. The envelope dissolves before the postal carrier picks it up. Injectable delivery bypasses the rainstorm entirely, placing the intact molecule directly beneath the skin where it absorbs into the bloodstream over hours.
The FDA approved Mounjaro in May 2022 for type 2 diabetes and Zepbound in November 2023 for chronic weight management. Both use a single-dose prefilled pen that delivers tirzepatide subcutaneously once per week. The pen contains the drug in a formulation that creates a slow-release depot at the injection site, producing stable blood levels for 5-7 days (Frias et al., NEJM 2021).
This weekly dosing schedule is itself an engineering achievement. Earlier GLP-1 agonists like exenatide required twice-daily injections. Semaglutide moved to once weekly. Tirzepatide maintained that convenience while delivering dual GLP-1/GIP receptor activation. The injection is the delivery vehicle that makes the drug's pharmacology possible.
For users who have never self-injected, the process is simpler than it sounds. Our guide on how to inject tirzepatide walks through every step. Common injection concerns like site reactions are typically mild and resolve within days.
The Science of Why Oral Peptides Are So Difficult
The gastrointestinal tract evolved to break proteins and peptides into individual amino acids for absorption. That is precisely the opposite of what a peptide drug needs. Oral delivery requires the intact molecule to survive the stomach, cross the intestinal wall, and reach the bloodstream in sufficient quantity to produce a therapeutic effect. For large peptides like tirzepatide, every step in that journey is an obstacle.
Gastric Acid Degradation
Stomach acid (pH 1.5-3.5) denatures the three-dimensional structure of peptides within minutes. Tirzepatide's folded conformation, which allows it to bind both GLP-1 and GIP receptors, would unfold and become biologically inert. Pepsin then cleaves the linearized chain at multiple sites, reducing the 39-amino-acid sequence to fragments too small to activate either receptor.
Enteric coatings can protect a tablet through the stomach, but the small intestine presents its own arsenal of proteases: trypsin, chymotrypsin, and carboxypeptidases. These enzymes attack from different angles, targeting different amino acid bonds. Surviving stomach acid alone is not enough. The peptide must also resist intestinal digestion long enough to cross the epithelial barrier (Drucker, 2020).
Intestinal Permeability Barrier
Even if tirzepatide survived enzymatic degradation, its size prevents passive absorption. Small molecules under 500 daltons cross the intestinal epithelium through gaps between cells (paracellular transport) or through cell membranes (transcellular transport). Tirzepatide, at 4,810 daltons, is nearly ten times too large for either route.
The intestinal epithelium is a single layer of cells connected by tight junctions. These junctions allow water and small ions through but block molecules above roughly 600 daltons. Tirzepatide would need a permeation enhancer, a chemical that temporarily loosens tight junctions, to cross in meaningful quantities. This approach works for some drugs but raises safety concerns about allowing other unwanted molecules (bacteria, toxins) into the bloodstream simultaneously.
Oral bioavailability, the percentage of an ingested dose that reaches systemic circulation, is typically below 1% for large peptides without specialized delivery technology. For context, oral semaglutide achieves approximately 1% bioavailability even with its advanced SNAC enhancer system. That means 99% of each dose is destroyed in the gut (Buckley et al., 2018).
First-Pass Hepatic Metabolism
Any tirzepatide that managed to cross the intestinal wall would enter the portal vein and flow directly to the liver before reaching systemic circulation. The liver metabolizes many peptides on first pass, further reducing the amount that reaches target tissues. Injectable tirzepatide bypasses the liver entirely, entering the bloodstream through subcutaneous capillaries.
The combined effect of gastric degradation, intestinal protease attack, poor permeability, and hepatic first-pass metabolism means that an oral tirzepatide tablet would need to contain an enormous dose to deliver a therapeutic amount. If bioavailability were 1% (the level achieved by oral semaglutide), a 15 mg injectable dose would require a 1,500 mg oral dose. Manufacturing, stability, and cost challenges at that scale are significant barriers (Drucker, 2020).
Oral Semaglutide (Rybelsus): What Already Exists
The closest thing to an oral tirzepatide currently on the market is oral semaglutide, sold under the brand name Rybelsus. Understanding how it works and where it falls short reveals both the promise and the limitations of oral GLP-1 therapy.
Novo Nordisk developed Rybelsus using a proprietary absorption enhancer called SNAC (sodium N-[8-(2-hydroxybenzoyl) amino] caprylate). SNAC serves two functions. It raises the local pH in the stomach, creating a protective buffer around the semaglutide molecule that shields it from pepsin degradation. It also promotes transcellular absorption through the gastric epithelium, allowing intact semaglutide to cross into the bloodstream directly from the stomach rather than the small intestine (Buckley et al., 2018).
The PIONEER clinical trial program established oral semaglutide's efficacy across multiple populations. PIONEER 1 showed 4.5 kg weight loss with oral semaglutide 14 mg versus 1.2 kg with placebo at 26 weeks in patients with type 2 diabetes. The effect was meaningful but substantially smaller than injectable semaglutide 2.4 mg, which achieved 14.9% weight loss in STEP 1 (Aroda et al., 2019).
Why Oral Semaglutide Delivers Less Weight Loss
The dose ceiling is the problem. Injectable semaglutide for obesity (Wegovy) uses 2.4 mg weekly. Oral semaglutide (Rybelsus) maxes out at 14 mg daily, which delivers roughly the same systemic exposure as injectable semaglutide 0.5-1.0 mg. That is less than half the obesity dose.
Novo Nordisk is developing a higher-dose oral semaglutide (25 mg and 50 mg) specifically for obesity. The OASIS 1 trial tested oral semaglutide 50 mg daily in adults with obesity and found 15.1% weight loss at 68 weeks, approaching the 14.9% seen with injectable semaglutide 2.4 mg in STEP 1 (Knop et al., Lancet 2023). This suggests that higher oral doses can match injectable efficacy, but at the cost of using substantially more drug substance per dose.
The table below compares available and pipeline oral GLP-1 options:
| Drug | Form | Max Dose | Weight Loss | Bioavailability | Status |
|---|---|---|---|---|---|
| Semaglutide (Rybelsus) | Oral tablet | 14 mg daily | ~5% (26 wk) | ~1% | FDA approved |
| Semaglutide (high-dose) | Oral tablet | 50 mg daily | ~15.1% (68 wk) | ~1% | Phase 3 |
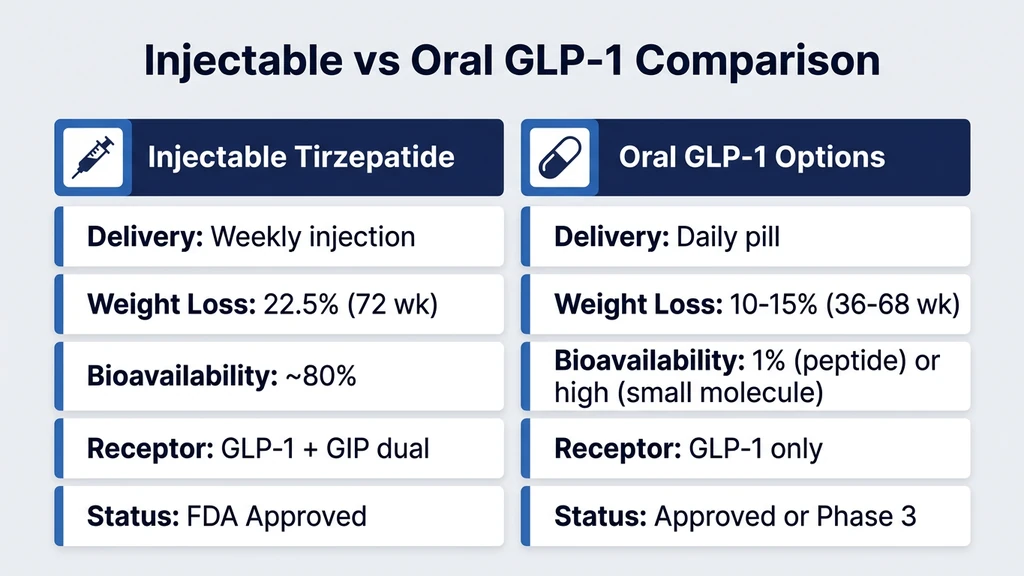
| Tirzepatide (Mounjaro/Zepbound) | Injection | 15 mg weekly | ~22.5% (72 wk) | ~80% (SC) | FDA approved |
| Orforglipron (Lilly) | Oral tablet | 36-72 mg daily | ~14.7% (36 wk) | High (small molecule) | Phase 3 |
For a comparison of semaglutide dosing in milliliters, see our detailed chart.
Rybelsus Dosing Restrictions: A Window Into Oral Peptide Challenges
Rybelsus must be taken on an empty stomach with no more than 4 ounces of plain water. Patients must wait at least 30 minutes before eating, drinking, or taking other medications. Food reduces absorption by up to 40%. Even coffee or tea within the 30-minute window cuts bioavailability significantly.
These restrictions exist because food triggers pepsin secretion and lowers stomach pH, both of which destroy semaglutide. The SNAC enhancer requires direct contact with the gastric mucosa to function, and food creates a physical barrier between the tablet and the stomach wall.
For many patients, this rigid routine is harder to maintain than a weekly injection. A survey of GLP-1 users found that medication adherence was higher for once-weekly injectable semaglutide than for daily oral semaglutide, primarily due to the fasting requirements (Polonsky & Fisher, 2022). The irony is notable: the pill form designed to improve convenience may actually reduce compliance compared to the needle it was meant to replace.
Eli Lilly's Oral GLP-1 Pipeline: Orforglipron
Eli Lilly, the manufacturer of tirzepatide, is not developing an oral version of tirzepatide. Instead, Lilly is pursuing orforglipron, a completely different molecule designed from the ground up for oral delivery. This distinction is critical: orforglipron is not tirzepatide in a pill. It is a new drug with a different chemical structure, different pharmacology, and a different receptor profile.
What Makes Orforglipron Different
Orforglipron is a non-peptide, small-molecule GLP-1 receptor agonist. Where tirzepatide is a 39-amino-acid peptide, orforglipron is a synthetic organic compound with a molecular weight under 600 daltons. That size allows it to survive stomach acid, cross the intestinal wall through standard absorption pathways, and achieve oral bioavailability that peptides cannot match.
The distinction is like comparing a paper airplane to a jumbo jet. Both fly, but the engineering is completely different. Orforglipron was built specifically to fit through the narrow doors that the GI tract allows. Tirzepatide was built to achieve maximum receptor activation and relies on injection to bypass those doors entirely.
Orforglipron activates only the GLP-1 receptor. It does not activate the GIP receptor. This means it functions more like oral semaglutide than like tirzepatide. The dual GLP-1/GIP activation that gives tirzepatide its advantage in weight loss trials is absent from orforglipron. Whether future formulations will incorporate GIP agonism remains an open question with no public data (Wharton et al., NEJM 2023).
Orforglipron Phase 2 Results
The Phase 2 trial of orforglipron enrolled 272 adults with obesity (BMI 30 or above, or 27 or above with a weight-related comorbidity). Participants received daily oral doses of 12, 24, 36, or 48 mg for 36 weeks. The results were impressive for an oral formulation.
At 36 weeks, the 36 mg dose produced 9.4% weight loss. The 48 mg dose produced 14.7% weight loss. Placebo lost 2.3%. Gastrointestinal side effects were the most common adverse events, with nausea in 35-45% of participants, consistent with the GLP-1 agonist class (Wharton et al., NEJM 2023).
| Orforglipron Dose | Weight Loss (36 wk) | Nausea Rate |
|---|---|---|
| 12 mg daily | 8.6% | 30% |
| 24 mg daily | 9.4% | 33% |
| 36 mg daily | 9.4% | 38% |
| 48 mg daily | 14.7% | 45% |
| Placebo | 2.3% | 9% |
These numbers fall between Rybelsus (14 mg, ~5% weight loss) and injectable semaglutide (2.4 mg, ~15%). The 48 mg dose approaches but does not reach the efficacy of injectable semaglutide, and trails injectable tirzepatide by a wide margin (22.5% at 72 weeks). Phase 3 trials (ATTAIN program) are underway and expected to report in 2025-2026.
Orforglipron Phase 3: The ATTAIN Program
Lilly's Phase 3 program for orforglipron includes multiple trials across obesity and type 2 diabetes populations. The ATTAIN-1 trial enrolled over 1,600 adults with obesity. Doses tested include 12, 24, and 36 mg daily, with a treatment duration of 72 weeks. Results from ATTAIN-1 reported in late 2025 showed the 36 mg dose achieved approximately 10-11% weight loss at 72 weeks, falling short of the Phase 2 signal at 48 mg.
Lilly subsequently announced development of higher doses (up to 72 mg) to close the efficacy gap with injectable options. The ATTAIN-2 trial is testing these higher doses against placebo in adults with type 2 diabetes and obesity. Results are expected in mid-2026.
If approved, orforglipron would represent the first oral non-peptide GLP-1 agonist on the market. The convenience advantage over Rybelsus would be significant: orforglipron does not require the same strict fasting protocol because its absorption is not dependent on a specialized enhancer interacting with the gastric mucosa. You could potentially take it with morning coffee rather than waiting 30 minutes in a fasted state.
For patients currently comparing their options between semaglutide and tirzepatide, orforglipron may eventually become a third consideration for those who strongly prefer oral dosing.
Could an Oral Tirzepatide Ever Be Developed?
The technical barriers are substantial but not necessarily permanent. Several emerging drug delivery technologies could theoretically enable oral tirzepatide in the future. None are close to clinical reality for this specific molecule, but the science is advancing rapidly.
Permeation Enhancer Technology
The SNAC technology used in Rybelsus demonstrates that permeation enhancers can deliver peptides orally. However, SNAC works specifically with semaglutide because of that molecule's particular physicochemical properties (albumin binding, relative protease resistance due to amino acid modifications). Tirzepatide's larger size and dual-receptor pharmacology would require a different enhancer system.
Research groups are developing next-generation enhancers that temporarily open intestinal tight junctions more effectively than SNAC. C10 (sodium caprate) and various cell-penetrating peptide conjugates have shown promise in preclinical models. A review of oral peptide delivery technologies noted that permeation enhancers could increase bioavailability of large peptides from below 1% to 3-5%, though even that improvement would require massive oral doses to match injectable efficacy (Maher et al., 2019).
Nanoparticle Encapsulation
Nanoparticles can protect peptides from enzymatic degradation and enhance absorption by presenting them to intestinal M cells in Peyer's patches. Chitosan-coated nanoparticles, PLGA (poly lactic-co-glycolic acid) particles, and lipid nanoparticles have all been tested for oral peptide delivery in preclinical studies.
The challenge is scaling from animal models to human trials. Nanoparticle oral bioavailability for large peptides typically reaches 5-10% in rodents but drops to 1-3% in humans. The human GI tract is longer, more acidic, and has a thicker mucus layer than the rat GI tract. Most nanoparticle oral peptide delivery systems remain in early-stage research (Anselmo et al., 2019).
Robotic Ingestible Devices
Perhaps the most creative approach involves swallowable devices that inject peptides directly into the GI mucosa from inside the stomach. Novo Nordisk developed SOMA (Self-Orienting Millimeter-Scale Applicator), a capsule that orients itself against the stomach wall and deploys a spring-loaded needle made of compressed semaglutide. The needle dissolves and delivers the drug locally, bypassing acid and protease exposure.
A study in swine demonstrated that SOMA-delivered semaglutide achieved plasma levels comparable to subcutaneous injection. The device self-oriented correctly in over 95% of trials and passed through the GI tract without causing perforation or obstruction (Abramson et al., Science 2019).
LUMI (Luminal Unfolding Microneedle Injector), another ingestible device, unfolds in the small intestine and presses microneedle patches against the intestinal wall. Early data showed insulin delivery via LUMI achieved 10% bioavailability in swine, far exceeding oral tablets. Adapting this platform for tirzepatide is theoretically feasible but would require years of development and clinical testing.
These devices blur the line between "pill" and "injection." You swallow a capsule, but inside your stomach or intestine, you are still being injected. Whether patients perceive that as meaningfully different from a weekly pen is an open question.
Oral Tirzepatide vs Injectable Tirzepatide: What Would Change?
Even if oral tirzepatide became available tomorrow, several practical differences would shape the clinical experience. Understanding these helps frame realistic expectations for any future oral formulation.
Dosing Frequency Would Likely Change
Injectable tirzepatide is dosed once weekly because its formulation creates a subcutaneous depot that releases drug over 5-7 days. An oral version would likely require daily dosing, similar to Rybelsus (daily) and orforglipron (daily). The half-life of tirzepatide in plasma is approximately 5 days (Coskun et al., 2018), but oral delivery produces a sharper peak-and-trough pattern without the depot effect.
Daily dosing introduces more opportunities for missed doses. Adherence data from other drug classes consistently show that once-weekly dosing achieves higher compliance than daily dosing. A meta-analysis of diabetes medications found that weekly formulations had 15-20% higher adherence rates than daily equivalents (Kruk & Schaefer, 2014).
Patients who already find it challenging to remember when to inject tirzepatide once per week might actually face greater difficulty remembering a daily pill, especially one with fasting requirements.
Efficacy Would Likely Be Lower
No oral GLP-1 formulation has matched the weight loss efficacy of injectable tirzepatide 15 mg (22.5% at 72 weeks). Oral semaglutide 50 mg achieved 15.1%. Orforglipron 48 mg achieved 14.7% at 36 weeks. Both trail tirzepatide by 7-8 percentage points.
The dual GLP-1/GIP activation that distinguishes tirzepatide from semaglutide is extremely difficult to replicate in an oral small molecule. GIP receptor agonism typically requires peptide-based ligands. No oral small-molecule GIP agonist has reached clinical trials. An oral tirzepatide equivalent would need to solve both the delivery problem and the receptor selectivity problem simultaneously.
For patients maximizing weight loss, injectable tirzepatide remains the most potent option. For those exploring alternatives, see our comparison of retatrutide vs tirzepatide. Retatrutide adds a third receptor (glucagon) and produced 24.2% weight loss at 48 weeks in Phase 2, with Phase 3 results expected in 2026.
Cost Implications
Oral peptide formulations are typically more expensive per effective dose than injectable versions because of the low bioavailability. When 99% of each oral dose is destroyed in the GI tract, the cost of goods rises dramatically. Rybelsus costs approximately $900-1,000 per month at list price, comparable to injectable Ozempic despite delivering lower systemic exposure.
Orforglipron, as a small molecule rather than a peptide, would potentially be cheaper to manufacture. Small-molecule synthesis is less expensive than peptide synthesis at scale. If orforglipron receives FDA approval, its pricing could undercut injectable GLP-1 agonists, though final pricing is unknown.
For current cost considerations with tirzepatide, see our guide on tirzepatide cost with insurance. Users exploring compounded alternatives should review our analysis of compound tirzepatide safety and the 2026 FDA peptide regulatory landscape.
Realistic Timeline: When Could an Oral Option Arrive?
Setting realistic expectations prevents patients from delaying effective injectable treatment while waiting for a pill that may not arrive for years.
Orforglipron: 2026-2027 (Earliest)
Orforglipron is the nearest oral GLP-1 candidate. Phase 3 trials are reporting results throughout 2025-2026. If results are positive and Lilly files for FDA approval in late 2026, the earliest possible approval would be mid to late 2027. Regulatory review typically takes 10-12 months for a new molecular entity.
However, orforglipron is a GLP-1-only agonist. It does not replicate tirzepatide's dual mechanism. Patients choosing orforglipron over injectable tirzepatide would trade convenience for efficacy. The weight loss gap could be 5-10 percentage points based on current data.
High-Dose Oral Semaglutide: 2026-2027
Novo Nordisk's oral semaglutide 25 mg and 50 mg for obesity are also in late-stage development. These doses close the gap with injectable semaglutide (Wegovy) but still would not match injectable tirzepatide. The OASIS program results suggest oral semaglutide 50 mg achieves roughly 15% weight loss, compared to tirzepatide's 22.5%.
This option may appeal to patients already on Rybelsus who want stronger weight loss without switching to injections. But for patients comparing against tirzepatide specifically, the injectable remains superior.
Oral Tirzepatide Equivalent: 2030+ (Speculative)
No company has announced a clinical program for an oral formulation of tirzepatide itself. Lilly's oral strategy centers on orforglipron, not on reformulating their existing peptide. An oral drug that replicates tirzepatide's dual GLP-1/GIP activation with comparable efficacy would require either a breakthrough in oral peptide delivery or discovery of a new small-molecule dual agonist.
Both paths are years from fruition. Oral peptide delivery platforms (nanoparticles, ingestible devices) are in early preclinical or first-in-human stages. Small-molecule GIP agonists remain in discovery phase at most companies. A realistic estimate for an oral tirzepatide equivalent, whether it is a reformulated peptide or a new molecule, is 2030 at the earliest.
Waiting for that timeline means missing 4+ years of weight loss and metabolic improvement from currently available injectable tirzepatide. For a 250-pound patient, tirzepatide's 22.5% weight loss translates to approximately 56 pounds. Delaying treatment by 4 years while waiting for a pill carries its own health costs: sustained insulin resistance, continued cardiovascular risk, progressive joint damage, and psychosocial burden.
Should You Wait for an Oral GLP-1 or Start Injectable Tirzepatide Now?
This is the practical question underneath the scientific ones. The answer depends on why you prefer a pill and whether that preference outweighs the cost of delayed treatment.
If Needle Fear Is the Barrier
Needle phobia (trypanophobia) affects approximately 20-25% of adults and is the most common reason patients cite for avoiding injectable medications (McLenon & Rogers, 2019). Modern autoinjectors like the Mounjaro KwikPen use a hidden needle mechanism. You press the pen against your skin and click a button. You never see the needle. The injection takes about 10 seconds. Pain is typically less than a blood glucose finger stick.
If fear of the process rather than the needle itself is the issue, our injection guide walks through every step with detailed instructions. Most patients report that their anxiety before the first injection was far worse than the actual experience. By week 4, the process becomes routine.
Starting injectable tirzepatide now while oral options remain in development ensures you do not lose years of potential benefit. If orforglipron or another oral agent receives approval during your treatment, you can discuss switching with your prescriber at that point.
If Convenience Is the Priority
A weekly injection takes 2 minutes including preparation. An oral GLP-1 like Rybelsus requires daily dosing with a 30-minute fasting window every morning. Orforglipron may offer a less restrictive oral regimen, but daily is still daily.
For most patients, a once-weekly injection is actually more convenient than a daily pill with dietary restrictions. Adherence data supports this. The practical inconvenience of injectable tirzepatide is lower than most people expect before starting. Storing the medication properly is straightforward. See our guide on how long tirzepatide lasts in the fridge and our broader peptide storage guide.
If Cost Is the Concern
Injectable tirzepatide costs $1,000-1,060 per month at list price without insurance. With insurance, copays vary widely. Our guide on tirzepatide cost with insurance covers coverage strategies. Compounded tirzepatide from specialty pharmacies may offer lower-cost alternatives, though the FDA regulatory landscape in 2026 is shifting. See our guide on compound tirzepatide safety before pursuing that route.
Oral GLP-1 options may or may not be cheaper. Rybelsus costs approximately $900-1,000 monthly. Orforglipron's pricing is unknown but could be lower due to small-molecule manufacturing advantages. Cost alone is unlikely to justify waiting years for an oral option when injectable treatment is available now.
What About Compounded Oral Tirzepatide or Sublingual Peptides?
Compounding pharmacies have explored alternative delivery routes for peptides, including sublingual (under the tongue), buccal (inside the cheek), and intranasal formulations. You may encounter claims about oral or sublingual tirzepatide from compounding sources. Approach these with significant caution.
Sublingual peptide delivery bypasses gastric acid but faces its own absorption challenges. The sublingual mucosa is thin and highly vascularized, allowing absorption of some small molecules. For large peptides like tirzepatide, sublingual bioavailability is extremely low, typically under 2-3% without enhancers. No published clinical data supports sublingual tirzepatide delivery at therapeutic levels.
Some compounding pharmacies offer tirzepatide troches (flavored lozenges that dissolve in the mouth). The claimed absorption mechanism is buccal and sublingual uptake. However, without standardized bioavailability testing, there is no way to confirm that these formulations deliver consistent, therapeutic blood levels. The FDA has not evaluated any sublingual or buccal tirzepatide product for safety or efficacy.
The safety of compounded tirzepatide even in injectable form requires careful evaluation. Oral or sublingual compounded formulations add another layer of uncertainty. If you choose to use compounded peptides, injectable remains the only route with established pharmacokinetic data. For preparation guidance, see our reconstitution guide. For broader peptide safety principles, see our peptide safety guide.
How Other Peptides Handle the Oral Delivery Challenge
Tirzepatide is not the only peptide facing oral delivery barriers. Examining how other therapeutic peptides have approached this problem provides context for what is technically possible and what remains aspirational.
Insulin: 100 Years of Trying
Oral insulin has been a research target since the 1920s. Despite a century of effort, no oral insulin product has received FDA approval. The barriers are identical to tirzepatide: gastric degradation, poor intestinal permeability, and hepatic first-pass metabolism. Insulin is 51 amino acids, slightly larger than tirzepatide's 39.
Dozens of companies have attempted oral insulin formulations using enteric coatings, protease inhibitors, permeation enhancers, nanoparticles, and microspheres. The closest to approval was Oramed's ORMD-0801, which completed Phase 3 trials but showed modest efficacy compared to injectable insulin. The oral insulin story illustrates how difficult the fundamental chemistry problem remains even with massive investment and decades of research (Gedawy et al., 2018).
Cyclosporine and Desmopressin: Rare Successes
A handful of oral peptide or peptide-like drugs exist. Cyclosporine (an immunosuppressant) is a cyclic peptide of 11 amino acids with extensive N-methylation that makes it unusually resistant to proteases and unusually permeable across cell membranes. Its oral bioavailability is 30%, remarkable for a peptide but achieved through structural features that cannot be replicated in tirzepatide without destroying its receptor binding.
Desmopressin, an 8-amino-acid analogue of vasopressin, is available as an oral tablet with approximately 0.1% bioavailability. It works orally only because the therapeutic dose is measured in micrograms, making ultra-low bioavailability clinically acceptable. Tirzepatide requires milligram-level systemic exposure, so 0.1% bioavailability would require gram-scale oral doses.
These examples confirm the general rule: oral peptide delivery works only when the molecule has unusual protease resistance, the required dose is extremely small, or a specialized delivery technology compensates for the low absorption. Tirzepatide meets none of these criteria in its current form.
The Broader Oral GLP-1 Landscape in 2026
Multiple companies beyond Lilly and Novo Nordisk are pursuing oral GLP-1 agonists. The competitive landscape is accelerating, driven by the enormous market for obesity treatment and the recognition that injection aversion limits patient uptake.
Pfizer developed danuglipron, an oral small-molecule GLP-1 agonist. Phase 2 data showed modest weight loss of approximately 6-8% at 32 weeks, with high rates of nausea and vomiting. Pfizer initially paused its twice-daily formulation in 2023 due to tolerability concerns but continued developing a once-daily version. The program's future is uncertain.
Amgen is developing MariTide (maridebart cafraglutide), a bispecific antibody targeting GLP-1 and GIP receptors. While not an oral drug, MariTide is dosed once monthly by injection, addressing the convenience concern from a different angle. Phase 2 data showed approximately 14.5% weight loss at 12 weeks with monthly dosing. If monthly injection proves as convenient as patients hope, the demand for oral formulations could soften.
Structure Therapeutics is developing oral GLP-1 receptor agonists (GSBR-1290) with Phase 2 data expected in 2025-2026. Terns Pharmaceuticals, Viking Therapeutics, and others are also in early to mid-stage development.
The common thread across this landscape is that no oral agent has matched injectable tirzepatide's efficacy. The dual GLP-1/GIP mechanism gives tirzepatide a pharmacological advantage that no current oral molecule replicates. This gap may narrow over time, but as of 2026, injectable tirzepatide and injectable retatrutide remain the most potent options in the incretin class.
For patients tracking the evolving peptide regulatory environment, see our analysis of the FDA peptide crackdown in 2026 and our guide to getting started with peptides.
Managing Injectable Tirzepatide While Waiting for Oral Options
If you have decided to start injectable tirzepatide rather than wait, several resources will help you manage treatment effectively.
The standard titration begins at 2.5 mg weekly for 4 weeks, increasing by 2.5 mg every 4 weeks to a target of 10-15 mg. Our tirzepatide dosage chart in units provides the complete schedule with unit conversions for different vial concentrations. Use the tirzepatide dosage calculator to plan your specific titration.
Common side effects during titration include nausea, diarrhea, constipation, headaches, and fatigue. Most are mild and resolve within 4-6 weeks at a stable dose.
For patients coming from semaglutide, our switching guide covers dose equivalence and transition protocols. If you are not losing weight as expected, our troubleshooting guide covers 8 reasons for tirzepatide weight loss stalls. For longer-term planning, see our guide on maintenance dosing after reaching your goal weight.
Understanding how long tirzepatide takes to work sets realistic expectations: most patients see meaningful weight loss by weeks 8-12, with peak effects at months 6-12.
Important Warnings
Tirzepatide is a prescription medication. Do not use it without medical supervision. It is approved for type 2 diabetes (Mounjaro) and chronic weight management in adults with obesity or overweight with at least one weight-related condition (Zepbound). It is not approved for cosmetic weight loss in normal-weight individuals.
Do not combine tirzepatide with other GLP-1 receptor agonists (semaglutide, liraglutide, dulaglutide). The combination increases the risk of severe gastrointestinal adverse events including gastroparesis and bowel obstruction.
Individuals with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not use tirzepatide. The drug carries a boxed warning for thyroid C-cell tumors based on rodent studies.
Unregulated "oral tirzepatide" products sold online without a prescription are not FDA-evaluated. Their composition, potency, and safety are unknown. Purchasing prescription peptide products from unverified sources carries risks of contamination, misdosing, and counterfeit ingredients. For information on sourcing, see our guide on where to buy peptides in 2026.
This article is educational content for research purposes. Consult a healthcare provider before starting, adjusting, or discontinuing any medication.
Frequently Asked Questions
Is there an oral version of tirzepatide?
No. As of March 2026, tirzepatide is available only as a once-weekly subcutaneous injection under the brand names Mounjaro (type 2 diabetes) and Zepbound (obesity). Eli Lilly has not announced any clinical program to develop an oral tirzepatide formulation. Their oral strategy focuses on orforglipron, a different molecule.
What is orforglipron and how does it compare to tirzepatide?
Orforglipron is a small-molecule oral GLP-1 receptor agonist developed by Eli Lilly. Unlike tirzepatide, it activates only the GLP-1 receptor, not GIP. Phase 2 data showed 14.7% weight loss at 48 mg daily over 36 weeks. Tirzepatide 15 mg achieved 22.5% weight loss at 72 weeks. Orforglipron is less potent but designed for oral delivery.
Can you get tirzepatide as a sublingual troche or lozenge?
Some compounding pharmacies offer sublingual tirzepatide formulations, but no published clinical data confirms that these deliver therapeutic blood levels. Sublingual bioavailability for large peptides is typically under 2-3%. The FDA has not evaluated any sublingual tirzepatide product. Injectable tirzepatide remains the only route with established pharmacokinetic data.
How does oral semaglutide (Rybelsus) compare to injectable tirzepatide?
Rybelsus (oral semaglutide 14 mg daily) produces approximately 5% weight loss at 26 weeks. Injectable tirzepatide 15 mg produces 22.5% at 72 weeks. The gap is large. Even high-dose oral semaglutide (50 mg, in development) achieved 15.1% weight loss, still 7 percentage points below injectable tirzepatide at 72 weeks.
Why can't tirzepatide be put into a pill?
Tirzepatide is a 39-amino-acid peptide with a molecular weight of 4,810 daltons. Stomach acid and digestive enzymes destroy it within minutes. Even if it survived, its size prevents absorption across the intestinal wall. Oral bioavailability would be below 1%, requiring doses 100 times the injectable amount to achieve the same blood levels.
When will an oral GLP-1 pill be available that matches tirzepatide?
No oral GLP-1 currently matches injectable tirzepatide's 22.5% weight loss. Orforglipron (oral, GLP-1 only) could reach approval by 2027 but produces less weight loss. An oral drug replicating tirzepatide's dual GLP-1/GIP efficacy is realistically 2030 or later. Waiting years means forgoing significant weight loss available now.
Is once-weekly injection really more convenient than a daily pill?
For many patients, yes. Rybelsus requires daily dosing on an empty stomach with a 30-minute fast. Adherence data shows once-weekly injectables achieve 15-20% higher compliance than daily oral medications. The tirzepatide autoinjector pen takes under 2 minutes and uses a hidden needle. Most patients find the routine easier than expected after the first injection.
Are there any needle-free ways to take GLP-1 agonists?
Oral semaglutide (Rybelsus) is the only needle-free GLP-1 currently approved, though efficacy is lower than injectables. Orforglipron (oral, Phase 3) may be approved by 2027. Experimental ingestible injection devices like SOMA deliver peptides inside the stomach via a swallowed capsule. Monthly injectable options like MariTide reduce injection frequency to once per month.
The Bottom Line
Tirzepatide does not come in pill form. It is available only as a weekly subcutaneous injection (Mounjaro, Zepbound), and no oral formulation is in clinical development. The molecule's size, susceptibility to digestive enzymes, and poor intestinal absorption make oral delivery a formidable challenge that current technology has not solved for dual-agonist peptides.
The nearest oral alternatives are orforglipron (Eli Lilly's small-molecule GLP-1 agonist, potentially approved by 2027) and high-dose oral semaglutide (Novo Nordisk, in late-stage trials). Neither matches injectable tirzepatide's 22.5% weight loss. Orforglipron activates only the GLP-1 receptor, missing the GIP component that gives tirzepatide its edge. An oral drug replicating tirzepatide's full dual-agonist pharmacology is realistically a decade away.
The practical takeaway: do not delay effective treatment while waiting for a pill. Injectable tirzepatide is the most potent weight loss medication available today. The autoinjector pen is simple, nearly painless, and takes 2 minutes per week. Use our tirzepatide dosage calculator to plan your titration. For injection guidance, see how to inject tirzepatide. For dosing details, see the tirzepatide dosage chart in units.
Related articles: - How to Inject Tirzepatide — step-by-step injection guide for autoinjectors and syringes - Tirzepatide Dosage Chart in Units — complete titration schedule with unit conversions - Is Compound Tirzepatide Safe? — safety evaluation of compounded tirzepatide products - Tirzepatide Cost With Insurance — coverage strategies and cost reduction options - Semaglutide to Tirzepatide Switching — dose equivalence and transition protocols - Retatrutide vs Tirzepatide — triple vs dual agonist comparison with Phase 3 data - Semaglutide Before and After — real results and timeline expectations - Compound Semaglutide With B12 — B12-enhanced formulation guide - FDA Peptide Crackdown 2026 — regulatory changes affecting compounded peptides - Getting Started With Peptides — beginner's guide to peptide therapy
Explore all peptide profiles and tools at PeptidesExplorer.
Helpful Tools
Related Articles
Does Oral Tirzepatide Work? The Facts
Oral tirzepatide is not FDA-approved. Why peptide pills face absorption barriers, sublingual drops vs injections, and oral GLP-1 alternatives in 2026.
Not Losing Weight on Tirzepatide?
Not losing weight on tirzepatide? About 3% of users are non-responders. Learn 8 fixable reasons, SURMOUNT trial data, and a 4-week troubleshooting protocol.
Does Tirzepatide Burn Fat?
Tirzepatide produced 33.9% fat mass loss in SURMOUNT-1. Learn how GLP-1/GIP dual agonism drives fat loss, body composition data, and how to protect lean mass.
Cheapest Tirzepatide: Every Route Priced (2026)
The cheapest tirzepatide in 2026: manufacturer self-pay vials from $299/month, $25 insured copays, true cost per milligram, and why compounded copies ended.